

Common musculoskeletal tumors of childhood and adolescence
- PMID: 22560526
- PMCID: PMC3538469
- DOI: 10.1016/j.mayocp.2012.01.015
Common musculoskeletal tumors of childhood and adolescence
Abstract
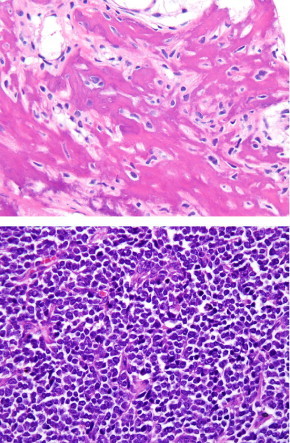
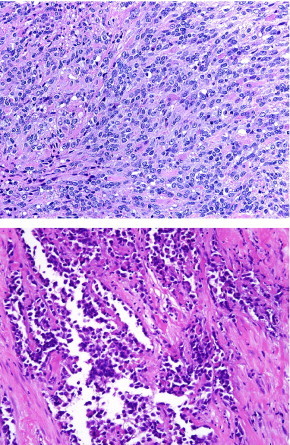
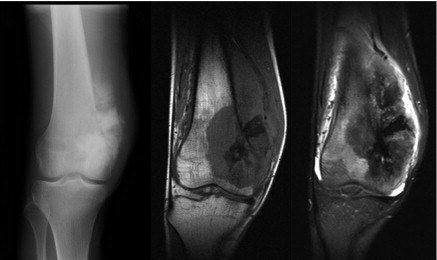
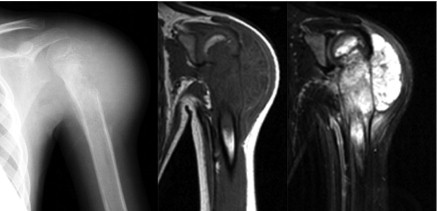
Osteosarcoma, Ewing sarcoma, and rhabdomyosarcoma are the most common malignant musculoskeletal tumors in children and adolescents. Today, most patients can be cured. Numerous factors have contributed to improved outcome for these patients over the past several decades. These include multidisciplinary care involving oncologists, radiation oncologists, surgeons, pathologists, and radiologists and enrollment of patients in clinical trials. Better understanding of molecular mechanisms of disease have resulted in studies using molecular targets in addition to standard chemotherapeutic agents, which hopefully will lead to better outcomes in the future. Moreover, new orthopedic techniques and devices as well as new technologies in radiation oncology hold promise for better local control of primary tumors and the potential for fewer late adverse effects. Despite this progress, patients must undergo lifelong follow-up for possible late effects of intense chemotherapy and radiation therapy. We review the diagnosis, prognosis, staging, multidisciplinary therapy, new directions in therapy, and long-term complications of treatment for these tumors. For this review, we searched MEDLINE using the terms rhabdomyosarcoma, osteosarcoma, Ewing sarcoma, biology, and humans and limited the search to articles from 2000 to September 2011. Additional references found in these articles were utilized as appropriate, as well as references from the background information in current therapeutic studies of the Children's Oncology Group. The same database and time frame were searched for articles written by leading authorities in the field.
Copyright © 2012 Mayo Foundation for Medical Education and Research. Published by Elsevier Inc. All rights reserved.
Figures

References
-
- Esiashvili N., Goodman M., Marcus R.B., Jr Changes in incidence and survival of Ewing sarcoma patients over the past 3 decades: Surveillance, Epidemiology, and End Results data. J Pediatr Hematol Oncol. 2008;30(6):425–430. - PubMed
-
- Mohseny A.B., Szuhai K., Romeo S. Osteosarcoma originates from mesenchymal stem cells in consequence of aneuploidization and genomic loss of Cdkn2. J Pathol. 2009;219(3):294–305. - PubMed
-
- Gorlick R. Current concepts on the molecular biology of osteosarcoma. Cancer Treat Res. 2009;152:467–478. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
