

In vivo detection of experimental optic neuritis by pupillometry
- PMID: 22561341
- PMCID: PMC3923364
- DOI: 10.1016/j.exer.2012.04.005
In vivo detection of experimental optic neuritis by pupillometry
Abstract
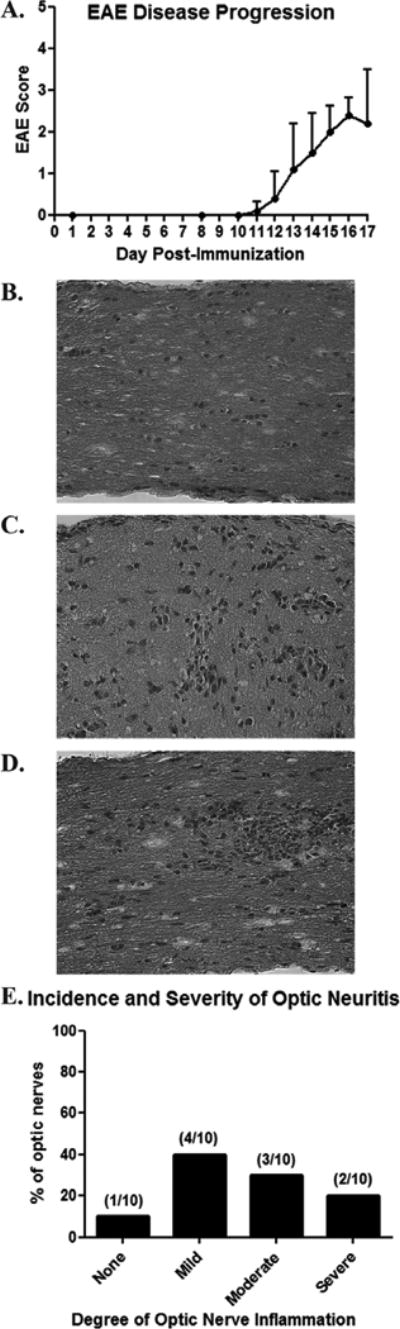
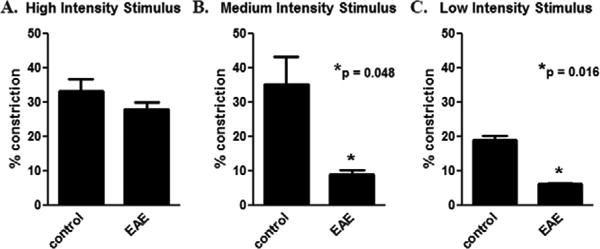
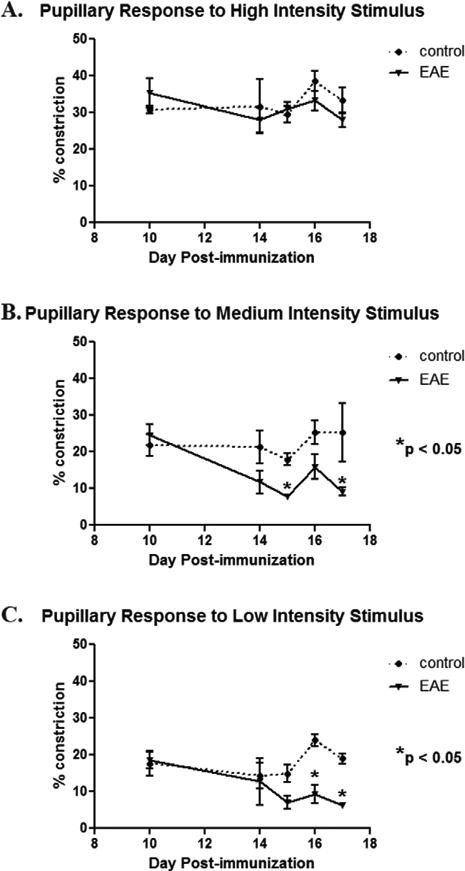
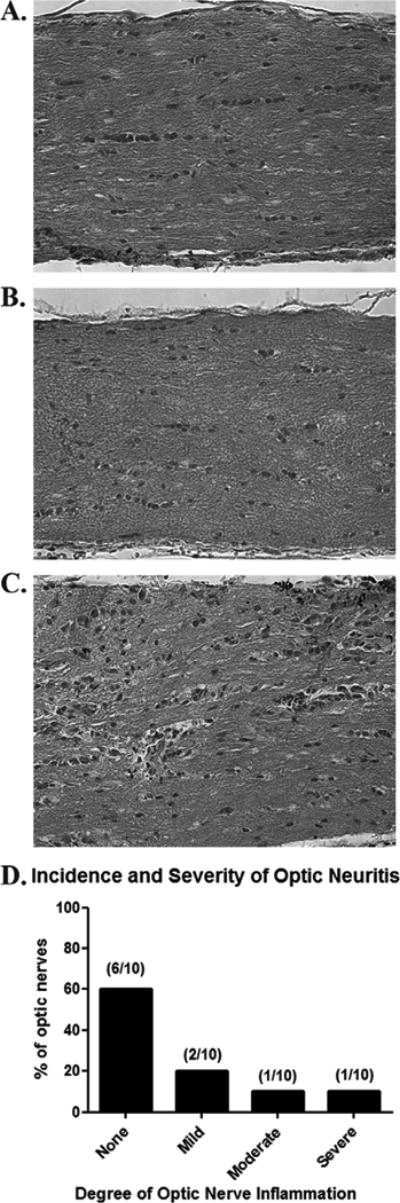
Optic neuritis is an inflammatory demyelination of optic nerve often occurring in multiple sclerosis (MS) patients. Mice with experimental autoimmune encephalomyelitis (EAE), an MS model, develop optic neuritis, but it is detected histologically after sacrifice, limiting the ability to monitor progression or treatment in vivo. We examined whether pupillary light responses measured by pupillometry can identify eyes with optic neuritis in EAE mice. C57BL/6 mice were exposed to unilateral light flashes of increasing intensity at 10 s intervals (4.7, 37, and 300 μW/cm(2)). Pupillary responses were recorded with a commercially available pupillometer. EAE was then induced by immunization with myelin oligodendrocyte glycoprotein. Pupillometry was repeated up to 17 days post-immunization, and responses were correlated with optic nerve inflammation. By day 17 post-immunization, 90% of EAE eyes had optic nerve inflammation. EAE eyes had significantly reduced pupillary constriction compared to control eyes. Mice exhibited more than a 25% decrease in pupillary constriction in at least one eye by days 13-15 post-immunization. In some eyes, pupil responses decreased prior to onset of detectable inflammation. Results show that pupillometry detects decreased optic nerve function in experimental optic neuritis, even in the absence of histological detection. Measuring pupillary constriction allows in vivo identification and functional assessment of eyes with optic neuritis that will be useful in evaluating potential therapies over time. Furthermore, results demonstrate that decreased visual function occurs early in optic neuritis, before optic nerve inflammation reaches its peak level.
Copyright © 2012 Elsevier Ltd. All rights reserved.
Figures
References
-
- Arnold AC. Evolving management of optic neuritis and multiple sclerosis. Am J Ophthalmol. 2005;139:1101–1108. - PubMed
-
- Beck RW, Cleary PA, Anderson MM, Jr, Keltner JL, Shults WT, Kaufman DI, Buckley EG, Corbett JJ, Kupersmith MJ, Miller NR, et al. A randomized, controlled trial of corticosteroids in the treatment of acute optic neuritis. New Eng J Med. 1992;326:581–588. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
