

A cost-utility analysis of transcatheter aortic valve implantation in Belgium: focusing on a well-defined and identifiable population
- PMID: 22561354
- PMCID: PMC3358616
- DOI: 10.1136/bmjopen-2012-001032
A cost-utility analysis of transcatheter aortic valve implantation in Belgium: focusing on a well-defined and identifiable population
Abstract
Background: Patients with severe aortic stenosis and coexisting non-cardiac conditions may be at high risk for surgical replacement of the aortic valve or even be no candidates for surgery. In these patients, transcatheter aortic valve implantation (TAVI) is suggested as an alternative. Results of the PARTNER (Placement of AoRTic TraNscathetER Valve) trial comparing the clinical effectiveness of TAVI with surgical valve replacement and standard therapy were published. The authors assessed the cost-effectiveness of TAVI in Belgium.
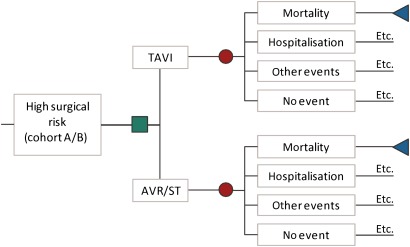
Methods: A Markov model of incremental costs, effects (survival and quality of life) and incremental cost-effectiveness of TAVI was developed. The impact on survival, number of events and quality of life was based on the PARTNER trial. Costs per event were context specific.
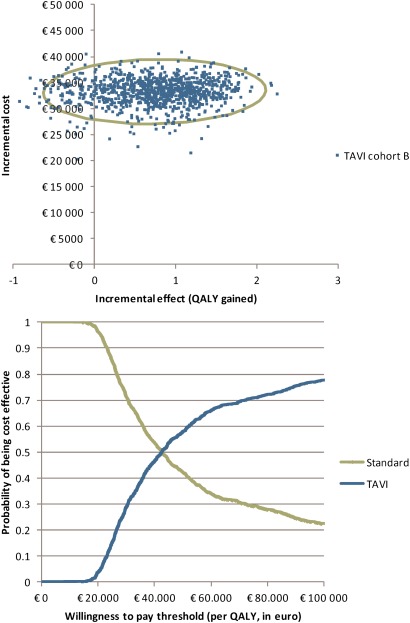
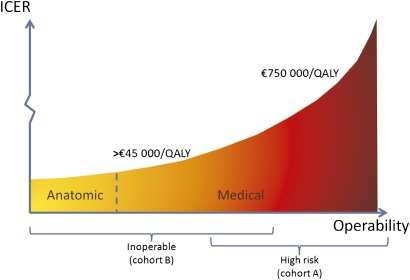
Results: In high-risk operable patients, even if the minor differences in 30-day and 1-year mortality are taken into account, the incremental cost-effectiveness ratio (ICER) remains on average above €750 000 per quality-adjusted life-year (QALY) gained (incremental cost: €20 400; incremental effect: 0.03 QALYs). In inoperable patients, an ICER of €44 900 per QALY (incremental cost: €33 200; incremental effect: 0.74 QALYs) is calculated, including a life-long extrapolation of the mortality benefit. This result was sensitive to the assumed time horizon. The subgroup of anatomically inoperable patients had better outcomes than medically inoperable patients, with ICERs decreasing more than €10 000/QALY.
Conclusions: It is inappropriate to consider reimbursement of TAVI for high-risk operable patients. Reimbursing TAVI in inoperable patients in essence is a political decision. From an economic perspective, it would be prudent to first target patients that are inoperable because of anatomical prohibitive conditions. In the search for evidence, the authors identified non-published negative results from a randomised controlled TAVI trial. The study sponsor should be more willing to share this information to allow balanced evaluations and policy recommendations. Payers should require these data before taking reimbursement decisions.
Conflict of interest statement
Figures
References
-
- Leon MB, Smith CR, Mack M, et al. Transcatheter aortic-valve implantation for aortic stenosis in patients who cannot undergo surgery. N Engl J Med 2010;363:1597–607 - PubMed
-
- Smith CR, Leon MB, Mack MJ, et al. Transcatheter versus surgical aortic-valve replacement in high-risk patients. N Engl J Med 2011;364:2187–98 - PubMed
-
- Cleemput I, Van Wilder P, Vrijens F, et al. Guidelines for Pharmacoeconomic Evaluations in Belgium. Health Technology Assessment (HTA). Brussels: Belgian Health Care Knowledge Centre (KCE), 2008
-
- FDA Meeting Materials of the Circulatory System Devices Panel. 2011. Department of Health and Human Services, Center for Devices and Radiological Health, Medical Devices Advisory Committee, Gaithersburg, Maryland, Washington DC, 20 July 2011. Annapolis, MD, USA: Free State Reporting, Inc., 2011
-
- Briggs A, Claxton K, Sculpher M. Decision Modelling for Health Economic Evaluation. Oxford: Oxford University Press, 2006
LinkOut - more resources
Full Text Sources