

Post-ablation prolongation of atrioventricular nodal refractory period is correlated with long-term success of cryoablation for atrioventricular nodal reentrant tachycardia in the case of the persistence of a residual jump
- PMID: 22562357
- PMCID: PMC3435514
- DOI: 10.1007/s10840-012-9680-7
Post-ablation prolongation of atrioventricular nodal refractory period is correlated with long-term success of cryoablation for atrioventricular nodal reentrant tachycardia in the case of the persistence of a residual jump
Abstract
Purpose: A residual slow pathway after successful cryoablation for atrioventricular nodal reentrant tachycardia (AVNRT) is correlated with a higher recurrence rate. We described determinants of recurrence in subjects with a residual jump.
Methods: We analyzed the data of subjects with acute successful slow pathway cryoablation for AVNRT using a 6-mm-tip cryocatheter. Success was defined as AVNRT non-inducibility. Patients with no baseline elicitable jump, no inducible AVNRT, and transient first atrioventricular (AV) block at the last site were excluded.
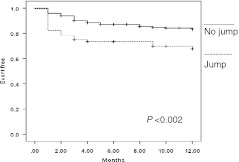
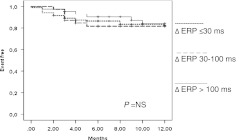
Results: From 371 patients who underwent cryoablation from May 2002 to March 2011, 303 fulfilled the entry criteria (mean age, 41 ± 16; 222 women). Baseline AV nodal effective refractory period (ERP) was 272 ± 57 ms, postprocedural 331 ± 64 (P < 0.001), and the mean of the difference (Δ ERP) 60 ± 41. At the end of the procedure, 64 patients (21 %) had a residual jump, of whom 22 with a single echo. At 12 months follow-up, the actuarial recurrence-free rate was 70.3 % in patients with a residual jump and 86 % in those without (P = 0.01). In patients with a jump, only Δ AV nodal ERP was correlated with recurrence (37 ± 41 vs. 68 ± 47 ms; P < 0.04) while a single echo was not. The actuarial rate of recurrence was 60.8 % in patients with a Δ AV nodal ERP ≤ 30 ms and 18.8 % in those with a Δ AV nodal ERP >30 ms (P < 0.01).
Conclusions: Suppression of slow pathway conduction is the optimal endpoint for AVNRT cryoablation. A residual jump can be tolerated if AV nodal ERP postcryoablation is prolonged >30 ms.
Figures

References
-
- De Sisti A, Tonet J. Cryoablation of atrioventricular nodal reentrant tachycardia: a clinical review. Pacing and Clinical Electrophysiology. 2011;10:1–8. - PubMed
-
- Stern JD, Rolnitzky L, Goldberg JD, Chinitz LA, Holmes DS, Bernstein NE, et al. Meta-analysis to assess the appropriate endpoint for slow pathway ablation of atrioventricular nodal reentrant tachycardia. Pacing and Clinical Electrophysiology. 2011;34:269–277. doi: 10.1111/j.1540-8159.2010.02948.x. - DOI - PubMed
-
- Gupta D, Al-Lamee RK, Earley MJ, Kistler P, Harris SJ, Nathan AW, et al. Cryoablation compared with radiofrequency ablation for atrioventricular nodal re-entrant tachycardia: analysis of factors contributing to acute and follow-up outcome. Europace. 2006;8:1022–1026. doi: 10.1093/europace/eul124. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
