

Urinary neutrophil gelatinase-associated lipocalin predicts mortality and identifies acute kidney injury in cirrhosis
- PMID: 22562534
- PMCID: PMC3979299
- DOI: 10.1007/s10620-012-2180-x
Urinary neutrophil gelatinase-associated lipocalin predicts mortality and identifies acute kidney injury in cirrhosis
Abstract
Background: Kidney failure predicts mortality in patients with cirrhosis. Identification of kidney failure etiology and recognition of those at the highest mortality risk remains a challenge.
Aims: We hypothesized that urinary neutrophil gelatinase-associated lipocalin (uNGAL) predicts mortality and identifies hepatorenal syndrome (HRS) in patients with cirrhosis.
Methods: Prospectively enrolled patients with cirrhosis were investigated by uNGAL immunoblot upon hospital admission. Kidney failure type was determined blinded to NGAL measurements.
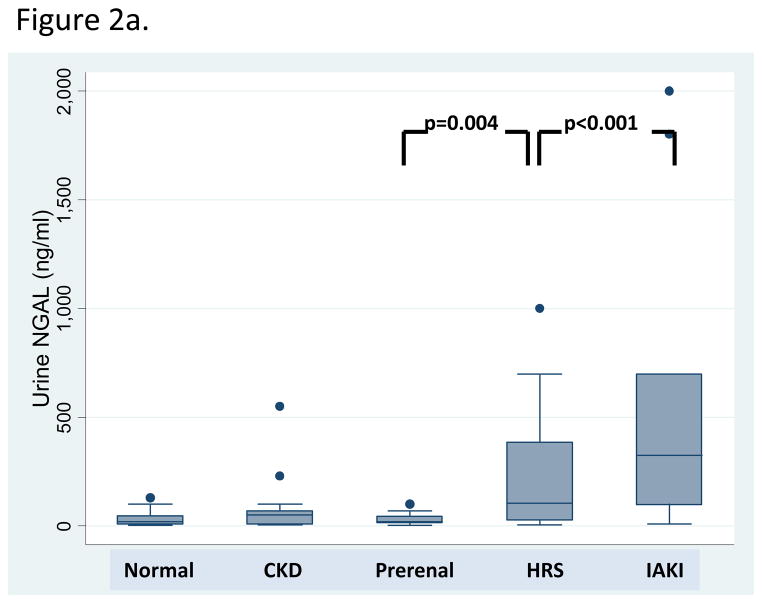
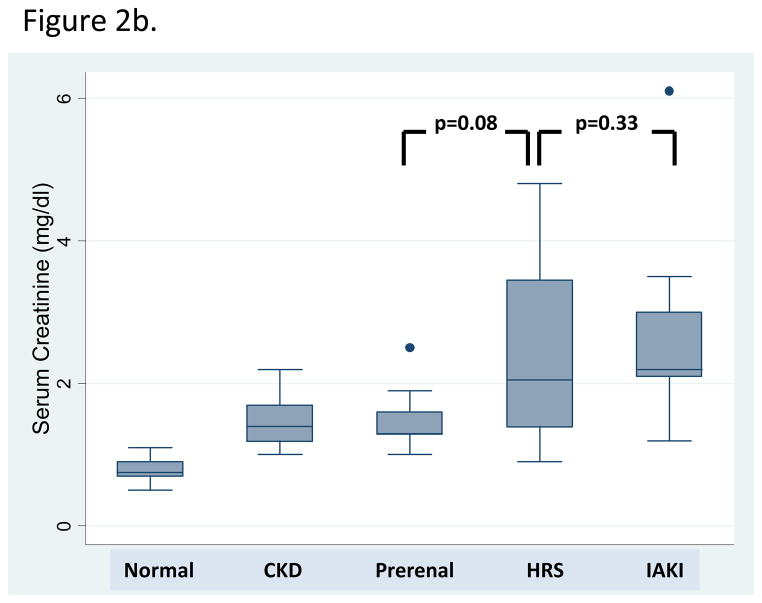
Results: One hundred eighteen patients were enrolled. Fifty-two (44 %) patients had normal kidney function, 14 (12 %) stable chronic kidney disease, 17 (14 %) prerenal azotemia, 20 (17 %) HRS, and 15 (13 %) intrinsic acute kidney injury (iAKI). Patients with HRS had uNGAL levels intermediate between prerenal azotemia [median (IQR) 105 (27.5-387.5) vs. 20 (15-45) ng/mL, p = 0.004] and iAKI [325 (100-700), p < 0.001]. Fifteen (13 %) patients died. In unadjusted analysis, uNGAL predicted inpatient mortality (OR 2.00, 95 % CI 1.36-2.94) and mortality or liver transplantation (OR 2.01, 95 % CI 1.42-2.85). In multiple regression models, uNGAL > 110 ng/mL (OR 6.05, 95 % CI 1.35-27.2) and HRS (OR 6.71, 95 % CI 1.76-25.5) independently predicted mortality, adjusting for age and serum creatinine >1.5 mg/dL.
Conclusions: uNGAL strongly predicts short-term inpatient mortality in both unadjusted and adjusted models. Patients with HRS may have uNGAL levels intermediate between those with prerenal azotemia and iAKI. Further studies are needed to determine if uNGAL can improve discrimination of HRS from other types of acute kidney injury and predict short- and long-term cirrhosis outcomes.
Figures
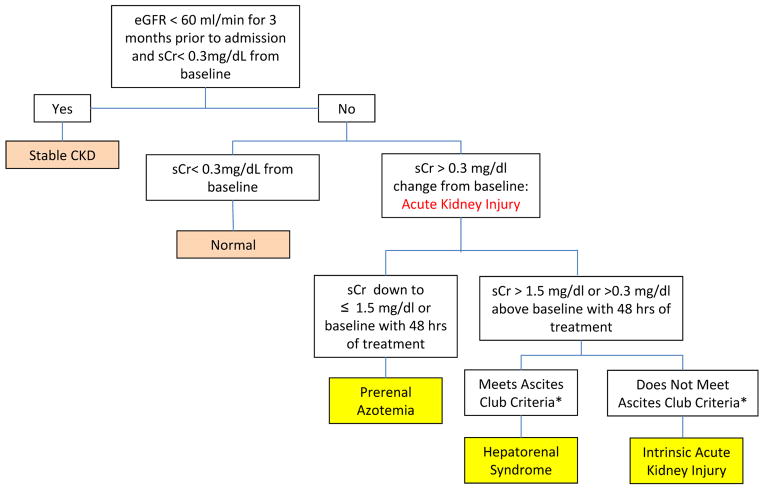
Presence of cirrhosis and ascites
sCr >1.5 mg/dL (or 133 micromoles/L)
No improvement of sCr (decrease equal to or less than 1.5 mg/dL) after at least 48 hours of diuretic withdrawal and volume expansion.
Absence of shock, current or recent treatment with nephrotoxic drugs
Absence of parenchymal kidney disease as indicated by proteinuria >500 mg/day, microhematuria (>50 RBCs/high power field, and/or abnormal renal ultrasound scanning
References
-
- Garcia-Tsao G, Parikh CR, Viola A. Acute kidney injury in cirrhosis. Hepatology. 2008;48:2064–2077. - PubMed
-
- Hampel H, Bynum GD, Zamora E, El-Serag HB. Risk factors for the development of renal dysfunction in hospitalized patients with cirrhosis. Am J Gastroenterol. 2001;96:2206–2210. - PubMed
-
- Terra C, Guevara M, Torre A, Gilabert R, Fernandez J, Martin-Llahi M, et al. Renal failure in patients with cirrhosis and sepsis unrelated to spontaneous bacterial peritonitis: value of MELD score. Gastroenterology. 2005;129:1944–1953. - PubMed
-
- du Cheyron D, Bouchet B, Parienti JJ, Ramakers M, Charbonneau P. The attributable mortality of acute renal failure in critically ill patients with liver cirrhosis. Intensive Care Med. 2005;31:1693–1699. - PubMed
-
- Wu CC, Yeung LK, Tsai WS, Tseng CF, Chu P, Huang TY, et al. Incidence and factors predictive of acute renal failure in patients with advanced liver cirrhosis. Clin Nephrol. 2006;65:28–33. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
