

Thoracolumbar intramedullary subependymoma with multiple cystic formation: a case report and review
- PMID: 22562689
- PMCID: PMC3641267
- DOI: 10.1007/s00586-012-2357-1
Thoracolumbar intramedullary subependymoma with multiple cystic formation: a case report and review
Abstract
Background: An intramedullary subependymoma is rare, particularly in the thoracolumbar region. Moreover, a radiographical obvious cystic formation of subependymoma of spinal cord rarely occurs in comparison to ependymoma.
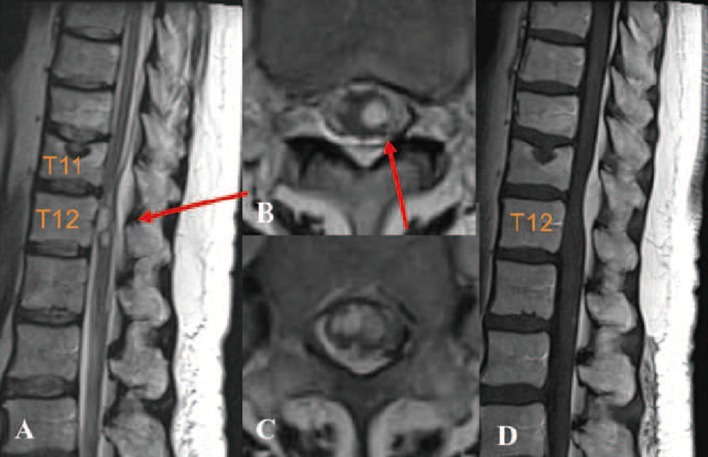
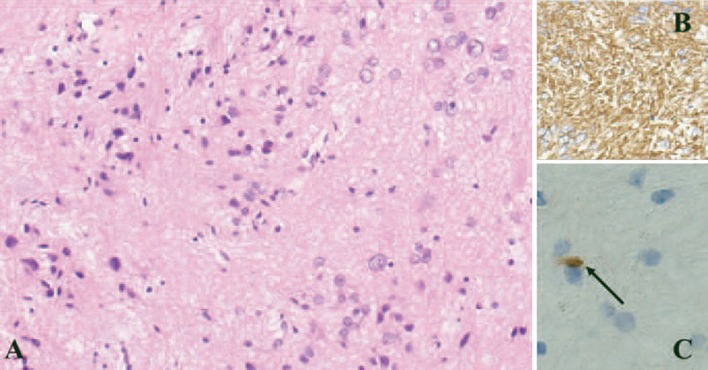
Case report: A 57-year-old woman presented with paraparesis. MRI revealed a multinodular and multicystic lesion in the spinal cord that was difficult to diagnose correctly. Intraoperative observation via midline myelotomy revealed a grayish, gelatinous solid mass with an eccentric localization. In addition, DREZtomy on the caudal side of the tumor revealed cystic formation. The cyst was punctured and xanthochromic fluid was collected. Attenuation of motor evoked potential (MEP) resulted in the partial removal of tumor. A pathological examination revealed the mass to be a subependymoma. The patient experienced transient worsening of symptoms, but improved gradually. No adjuvant radiosurgery was administered. Follow-up estimation 30 months after surgery revealed no evidences of regrowth.
Conclusions: This report presents this rare case, a review of the literature associated with thoracolumbar subependymomas, and a discussion of the clinical and radiographical characteristics.
Figures
References
-
- Iwasaki Y, Hida K (2006) The basic textbook of spinal surgery. Japan pp 168–170 (Japanese)
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
