

Prophylactic rituximab after allogeneic transplantation decreases B-cell alloimmunity with low chronic GVHD incidence
- PMID: 22563089
- PMCID: PMC3383022
- DOI: 10.1182/blood-2011-12-395970
Prophylactic rituximab after allogeneic transplantation decreases B-cell alloimmunity with low chronic GVHD incidence
Abstract
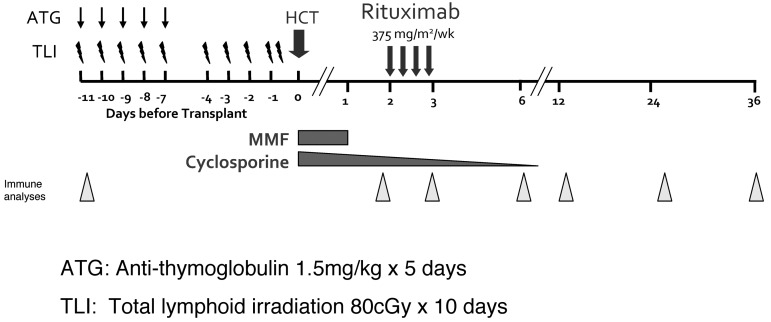
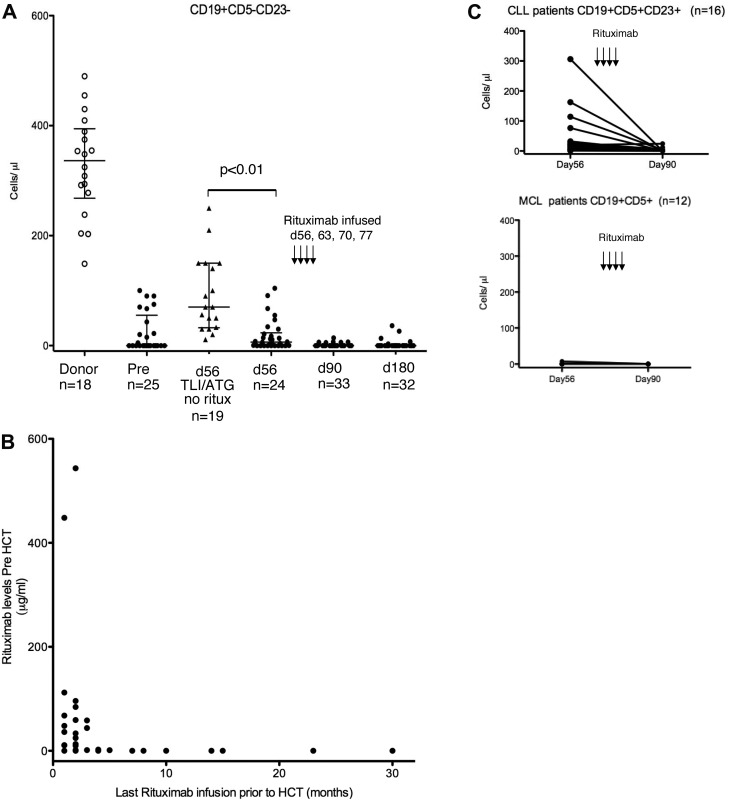
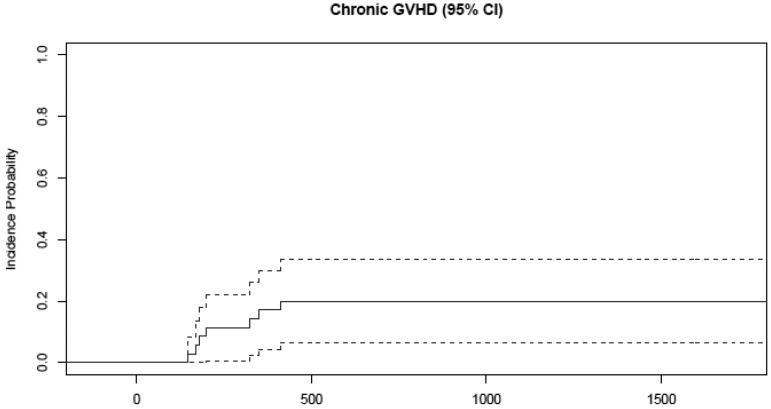
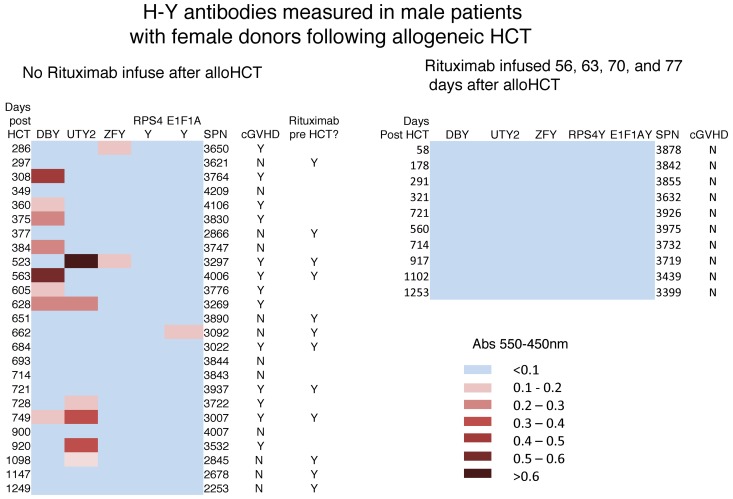
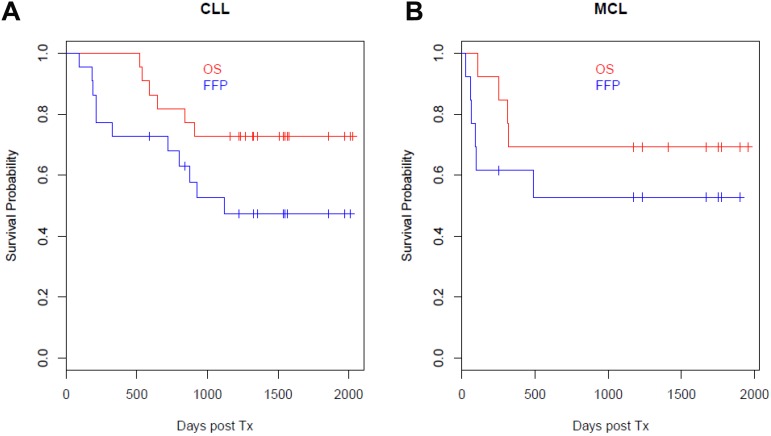
B cells are involved in the pathogenesis of chronic GVHD (cGVHD). We hypothesized that prophylactic anti-B-cell therapy delivered 2 months after transplantation would decrease allogeneic donor B-cell immunity and possibly the incidence of cGVHD. Therefore, in the present study, patients with high-risk chronic lymphocytic leukemia (n = 22) and mantle-cell lymphoma (n = 13) received a total lymphoid irradiation of 80 cGy for 10 days and antithymocyte globulin 1.5 mg/kg/d for 5 days. Rituximab (375 mg/m(2)) was infused weekly on days 56, 63, 70, and 77 after transplantation. The incidence of acute GVHD was 6%. The cumulative incidence of cGVHD was 20%. Nonrelapse mortality was 3%. Rituximab treatment after allogeneic transplantation significantly reduced B-cell allogeneic immunity, with complete prevention of alloreactive H-Y Ab development in male patients with female donors (P = .01). Overall survival and freedom from progression at 4 years for chronic lymphocytic leukemia patients were 73% and 47%, respectively; for mantle-cell lymphoma patients, they were 69% and 53%, respectively.
Trial registration: ClinicalTrials.gov NCT00186628.
Figures
References
-
- Lönnqvist B, Aschan J, Ljungman P, Ringden O. Long-term cyclosporin therapy may decrease the risk of chronic graft-versus-host disease. Br J Haematol. 1990;74(4):547–548. - PubMed
-
- Nash RA, Antin JH, Karanes C, et al. Phase 3 study comparing methotrexate and tacrolimus with methotrexate and cyclosporine for prophylaxis of acute graft-versus-host disease after marrow transplantation from unrelated donors. Blood. 2000;96(6):2062–2068. - PubMed
-
- Kansu E, Gooley T, Flowers ME, et al. Administration of cyclosporine for 24 months compared with 6 months for prevention of chronic graft-versus-host disease: a prospective randomized clinical trial. Blood. 2001;98(13):3868–3870. - PubMed
-
- Socié G, Schmoor C, Bethge WA, et al. Chronic graft-versus-host disease: long-term results from a randomized trial on graft-versus-host disease with or without anti-T-cell globulin ATG-Fresenius. Blood. 2011;117(23):6375–6382. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
