

Risk of cardiovascular serious adverse events associated with varenicline use for tobacco cessation: systematic review and meta-analysis
- PMID: 22563098
- PMCID: PMC3344735
- DOI: 10.1136/bmj.e2856
Risk of cardiovascular serious adverse events associated with varenicline use for tobacco cessation: systematic review and meta-analysis
Abstract
Objective: To examine the risk of treatment emergent, cardiovascular serious adverse events associated with varenicline use for tobacco cessation.
Design: Meta-analysis comparing study effects using four summary estimates.
Data sources: Medline, Cochrane Library, online clinical trials registries, and reference lists of identified articles.
Review methods: We included randomised controlled trials of current tobacco users of adult age comparing use of varenicline with an inactive control and reporting adverse events. We defined treatment emergent, cardiovascular serious adverse events as occurring during drug treatment or within 30 days of discontinuation, and included any ischaemic or arrhythmic adverse cardiovascular event (myocardial infarction, unstable angina, coronary revascularisation, coronary artery disease, arrhythmias, transient ischaemic attacks, stroke, sudden death or cardiovascular related death, or congestive heart failure).
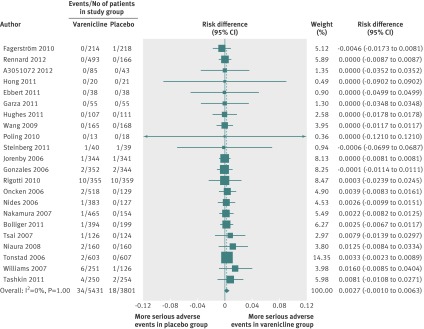
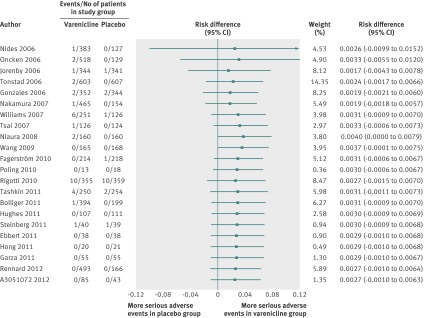
Results: We identified 22 trials; all were double blinded and placebo controlled; two included participants with active cardiovascular disease and 11 enrolled participants with a history of cardiovascular disease. Rates of treatment emergent, cardiovascular serious adverse events were 0.63% (34/5431) in the varenicline groups and 0.47% (18/3801) in the placebo groups. The summary estimate for the risk difference, 0.27% (95% confidence interval -0.10 to 0.63; P = 0.15), based on all 22 trials, was neither clinically nor statistically significant. For comparison, the relative risk (1.40, 0.82 to 2.39; P = 0.22), Mantel-Haenszel odds ratio (1.41, 0.82 to 2.42; P = 0.22), and Peto odds ratio (1.58, 0.90 to 2.76; P = 0.11), all based on 14 trials with at least one event, also indicated a non-significant difference between varenicline and placebo groups.
Conclusions: This meta--analysis--which included all trials published to date, focused on events occurring during drug exposure, and analysed findings using four summary estimates-found no significant increase in cardiovascular serious adverse events associated with varenicline use. For rare outcomes, summary estimates based on absolute effects are recommended and estimates based on the Peto odds ratio should be avoided.
Conflict of interest statement
Competing interests: All authors have completed the Unified Competing Interest form at
Figures
Comment in
-
Flaws in analysis lead to misleading conclusions about varenicline's safety in smoking cessation.BMJ. 2012 Jun 12;344:e3873; author reply e4033. doi: 10.1136/bmj.e3873. BMJ. 2012. PMID: 22693049 No abstract available.
-
ACP Journal Club: review: varenicline for tobacco cessation does not increase CV serious adverse events.Ann Intern Med. 2012 Aug 21;157(4):JC2-2. doi: 10.7326/0003-4819-157-4-201208210-02002. Ann Intern Med. 2012. PMID: 22910956 No abstract available.
-
[Varenicline is a safe drug for smoking cessation].Praxis (Bern 1994). 2012 Aug 22;101(17):1128-9. doi: 10.1024/1661-8157/a001046. Praxis (Bern 1994). 2012. PMID: 22915518 German. No abstract available.
-
Varenicline's adverse events. Choice of summary statistics: relative and absolute measures.BMJ. 2013 Feb 26;346:f1092. doi: 10.1136/bmj.f1092. BMJ. 2013. PMID: 23444433 No abstract available.
References
-
- Centers for Disease Control and Prevention. Smoking-attributable mortality, years of potential life lost, and productivity losses—United States, 2000-2004. MMWR Morb Mortal Wkly Rep 2008;57:1226-8. - PubMed
-
- US Department of Health and Human Services. The health consequences of smoking: a report of the Surgeon General. US Department of Health and Human Services, 2004. www.surgeongeneral.gov/library/smokingconsequences/.
-
- Critchley JA, Capewell S. Mortality risk reduction associated with smoking cessation in patients with coronary heart disease: a systematic review. JAMA 2003;290:86-97. - PubMed
-
- Critchley J, Capewell S. Smoking cessation for the secondary prevention of coronary heart disease. Cochrane Database Syst Rev 2003:CD003041. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Molecular Biology Databases