

The effect of elevated body mass index on ischemic heart disease risk: causal estimates from a Mendelian randomisation approach
- PMID: 22563304
- PMCID: PMC3341326
- DOI: 10.1371/journal.pmed.1001212
The effect of elevated body mass index on ischemic heart disease risk: causal estimates from a Mendelian randomisation approach
Abstract
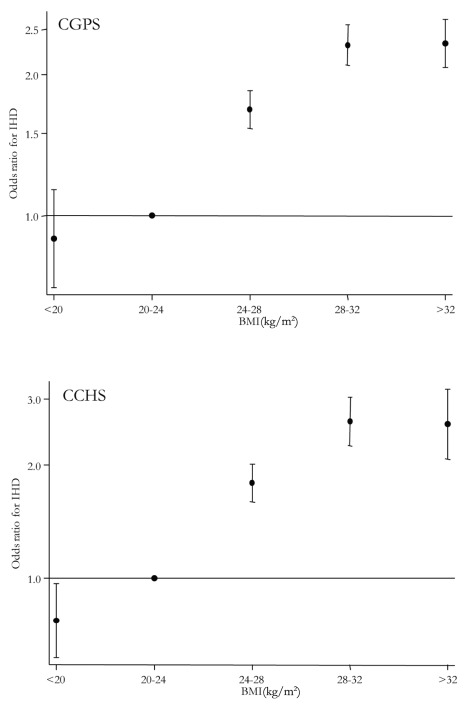
Background: Adiposity, assessed as elevated body mass index (BMI), is associated with increased risk of ischemic heart disease (IHD); however, whether this is causal is unknown. We tested the hypothesis that positive observational associations between BMI and IHD are causal.
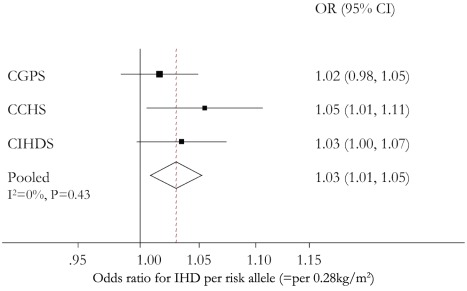
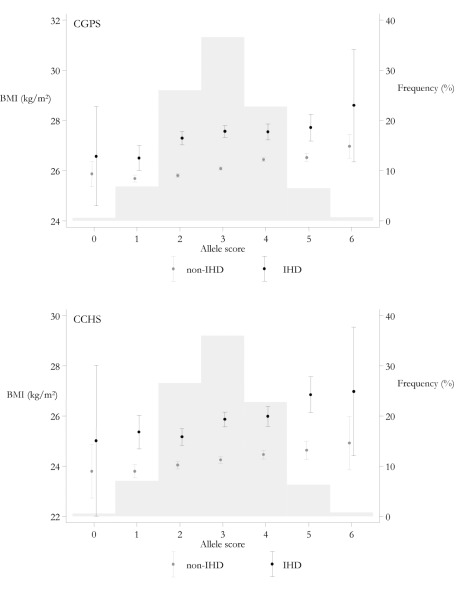
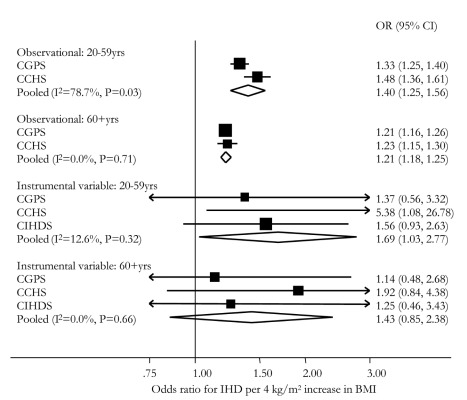
Methods and findings: In 75,627 individuals taken from two population-based and one case-control study in Copenhagen, we measured BMI, ascertained 11,056 IHD events, and genotyped FTO(rs9939609), MC4R(rs17782313), and TMEM18(rs6548238). Using genotypes as a combined allele score in instrumental variable analyses, the causal odds ratio (OR) between BMI and IHD was estimated and compared with observational estimates. The allele score-BMI and the allele score-IHD associations used to estimate the causal OR were also calculated individually. In observational analyses the OR for IHD was 1.26 (95% CI 1.19-1.34) for every 4 kg/m(2) increase in BMI. A one-unit allele score increase associated with a 0.28 kg/m(2) (95 CI% 0.20-0.36) increase in BMI and an OR for IHD of 1.03 (95% CI 1.01-1.05) (corresponding to an average 1.68 kg/m(2) BMI increase and 18% increase in the odds of IHD for those carrying all six BMI increasing alleles). In instrumental variable analysis using the same allele score the causal IHD OR for a 4 kg/m(2) increase in BMI was 1.52 (95% CI 1.12-2.05).
Conclusions: For every 4 kg/m(2) increase in BMI, observational estimates suggested a 26% increase in odds for IHD while causal estimates suggested a 52% increase. These data add evidence to support a causal link between increased BMI and IHD risk, though the mechanism may ultimately be through intermediate factors like hypertension, dyslipidemia, and type 2 diabetes. This work has important policy implications for public health, given the continuous nature of the BMI-IHD association and the modifiable nature of BMI. This analysis demonstrates the value of observational studies and their ability to provide unbiased results through inclusion of genetic data avoiding confounding, reverse causation, and bias.
Conflict of interest statement
George Davey Smith is on the
Figures


References
-
- Manson JE, Colditz GA, Stampfer MJ, Willett WC, Rosner B, et al. A prospective study of obesity and risk of coronary heart disease in women. N Engl J Med. 1990;322:882–889. - PubMed
-
- Ni Mhurchu C, Rodgers A, Pan WH, Gu DF, Woodward M, et al. Body mass index and cardiovascular disease in the Asia-Pacific Region: an overview of 33 cohorts involving 310 000 participants. Int J Epidemiol. 2004;33:751–758. - PubMed
-
- Kurth T, Gaziano JM, Rexrode KM, Kase CS, Cook NR, et al. Prospective study of body mass index and risk of stroke in apparently healthy women. Circulation. 2005;111:1992–1998. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
