

The impact of early monitored management on survival in hospitalized adult Ugandan patients with severe sepsis: a prospective intervention study*
- PMID: 22564958
- PMCID: PMC3378757
- DOI: 10.1097/CCM.0b013e31824e65d7
The impact of early monitored management on survival in hospitalized adult Ugandan patients with severe sepsis: a prospective intervention study*
Abstract
In sub-Saharan Africa, sepsis is an important cause of mortality. Optimal sepsis management including fluid resuscitation, early antibiotic administration, and patient monitoring is limited by lack of supplies and skilled health workers.
Objective: To evaluate whether early, monitored sepsis management provided by a study medical officer can improve survival among patients with severe sepsis admitted to two public hospitals in Uganda.
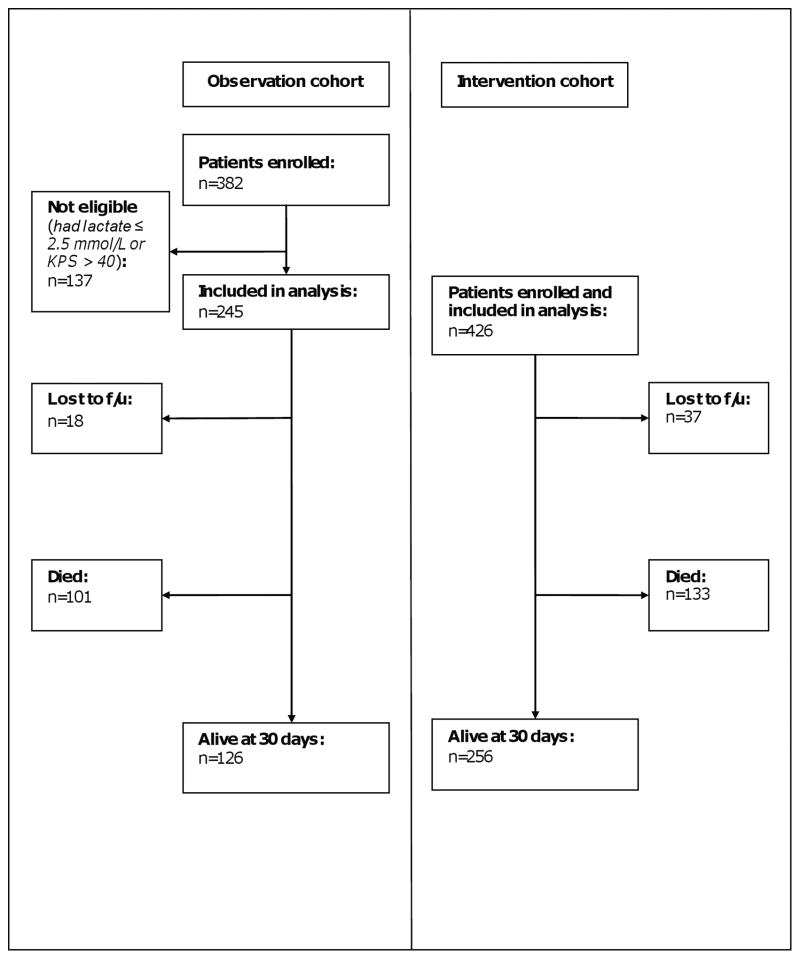
Design, setting, and patients: A prospective before and after study of an intervention cohort (n = 426) with severe sepsis receiving early, monitored sepsis management compared to an observation cohort (n = 245) of similarly ill patients with severe sepsis receiving standard management after admission to the medical wards of two Ugandan hospitals.
Intervention: Early sepsis management provided by a dedicated study medical officer comprising fluid resuscitation, early antibiotics, and regular monitoring in the first 6 hrs of hospitalization.
Measurements: Kaplan-Meier survival and unadjusted and adjusted Cox proportional hazards analysis were used to compare the effect of early, monitored sepsis management on 30-day mortality between the intervention cohort (enrolled May 2008 to May 2009) and observation cohort (enrolled July 2006 to November 2006).
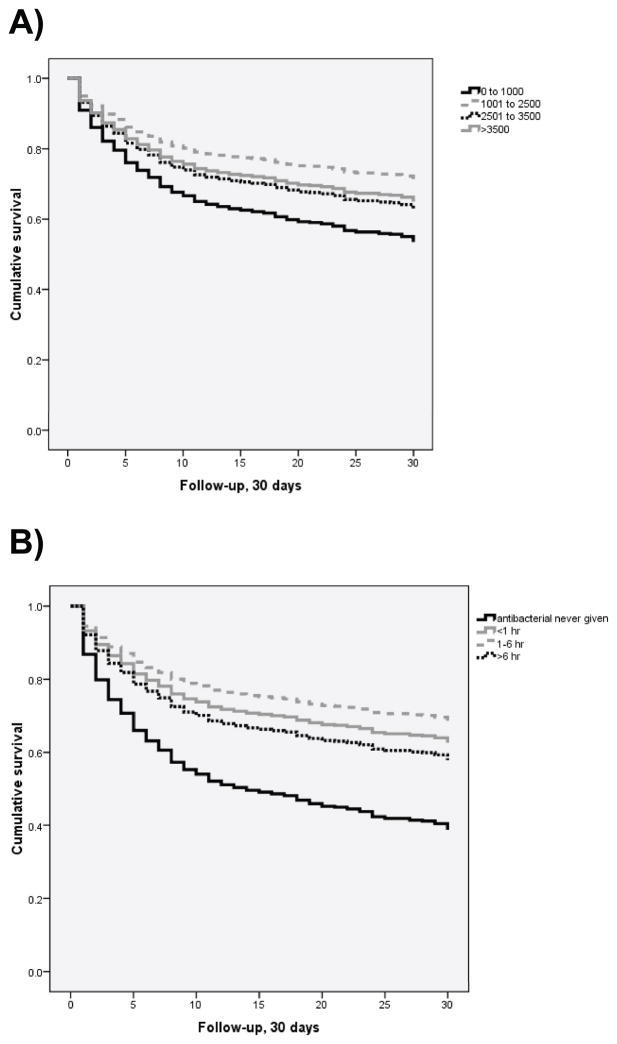
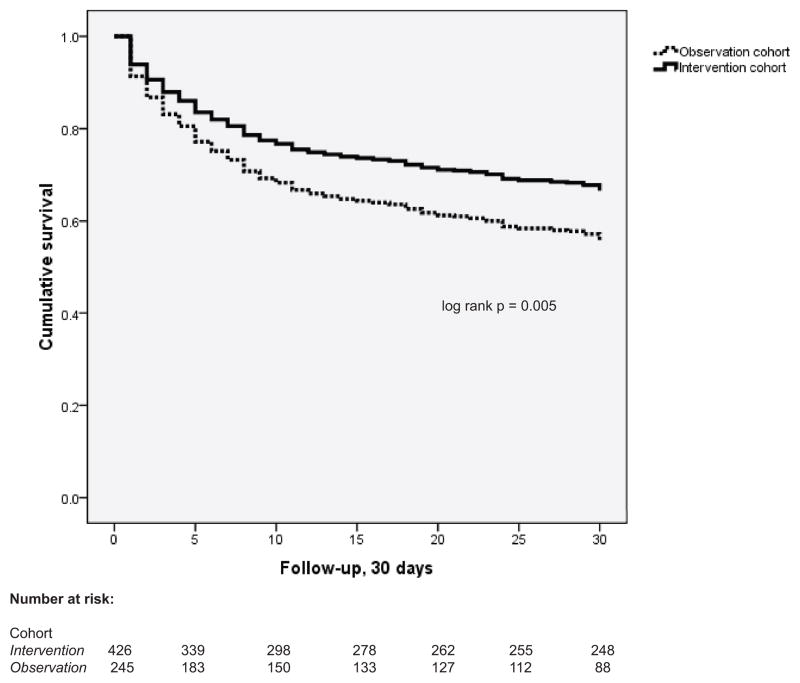
Results: The majority (86%) of patients in both cohorts were human immuno-deficiency virus-infected. Median fluid volume provided in the first 6 hrs of hospitalization was higher in intervention than observation cohort patients (3000 mL vs. 500 mL, p < .001) and a greater proportion of intervention cohort patients received antibacterial therapy in <1 hr (67% vs. 30.4%, p < .001). Mortality at 30 days was significantly lower in the intervention cohort compared to the observation cohort (33.0% vs. 45.7%, log-rank p = .005). After adjustment for potential confounders, the hazard of 30-day mortality was 26% less in the intervention cohort compared to the observation cohort (adjusted hazards ratio 0.74, 95% confidence interval 0.55-0.98). Mortality among the 13% of intervention patients who developed signs of respiratory distress was associated with baseline illness severity rather than fluid volume administered.
Conclusion: Early, monitored management of severely septic patients in Uganda improves survival and is feasible and safe even in a busy public referral hospital.
Conflict of interest statement
The authors have not disclosed any potential conflicts of interest
Figures
Comment in
-
Improving sepsis care in resource limited settings*.Crit Care Med. 2012 Jul;40(7):2234-6. doi: 10.1097/CCM.0b013e3182515068. Crit Care Med. 2012. PMID: 22710211 No abstract available.
References
-
- World Health Organization. The Global Burden of Disease: 2004 update. 2008 [cited 2010 28 July]; Available from: http://www.who.int/healthinfo/global_burden_disease/2004_report_update/e....
-
- Becker JU, Theodosis C, Jacob ST, Wira CR, Groce NE. Surviving sepsis in low-income and middle-income countries: new directions for care and research. Lancet Infect Dis. 2009;9(9):577–82. Epub 2009/08/22. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
