

Tobacco smoking and increased risk of death and progression for patients with p16-positive and p16-negative oropharyngeal cancer
- PMID: 22565003
- PMCID: PMC3397696
- DOI: 10.1200/JCO.2011.38.4099
Tobacco smoking and increased risk of death and progression for patients with p16-positive and p16-negative oropharyngeal cancer
Abstract
Purpose: Tobacco smoking is associated with oropharynx cancer survival, but to what extent cancer progression or death increases with increasing tobacco exposure is unknown.
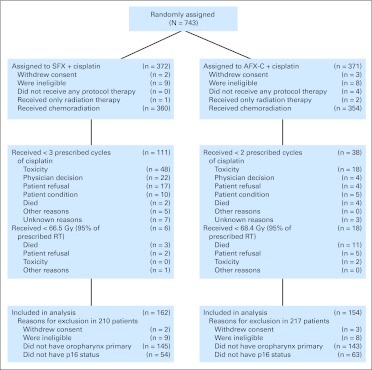
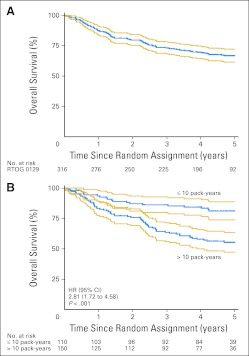
Patients and methods: Patients with oropharynx cancer enrolled onto a phase III trial of radiotherapy from 1991 to 1997 (Radiation Therapy Oncology Group [RTOG] 9003) or of chemoradiotherapy from 2002 to 2005 (RTOG 0129) were evaluated for tumor human papillomavirus status by a surrogate, p16 immunohistochemistry, and for tobacco exposure by a standardized questionnaire. Associations between tobacco exposure and overall survival (OS) and progression-free survival (PFS) were estimated by Cox proportional hazards models.
Results: Prevalence of p16-positive cancer was 39.5% among patients in RTOG 9003 and 68.0% in RTOG 0129. Median pack-years of tobacco smoking were lower among p16-positive than p16-negative patients in both trials (RTOG 9003: 29 v 45.9 pack-years; P = .02; RTOG 0129: 10 v 40 pack-years; P < .001). After adjustment for p16 and other factors, risk of progression (PFS) or death (OS) increased by 1% per pack-year (for both, hazard ratio [HR], 1.01; 95% CI, 1.00 to 1.01; P = .002) or 2% per year of smoking (for both, HR, 1.02; 95% CI, 1.01 to 1.03; P < .001) in both trials. In RTOG 9003, risk of death doubled (HR, 2.19; 95% CI, 1.46 to 3.28) among those who smoked during radiotherapy after accounting for pack-years and other factors, and risk of second primary tumors increased by 1.5% per pack-year (HR, 1.015; 95% CI, 1.005 to 1.026).
Conclusion: Risk of oropharyngeal cancer progression and death increases directly as a function of tobacco exposure at diagnosis and during therapy and is independent of tumor p16 status and treatment.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures


Comment in
-
Methodologic barriers to addressing critical questions about tobacco and cancer prognosis.J Clin Oncol. 2012 Jun 10;30(17):2030-2. doi: 10.1200/JCO.2012.41.7402. Epub 2012 May 7. J Clin Oncol. 2012. PMID: 22564998 No abstract available.
References
-
- Fountzilas G, Kosmidis P, Avramidis V, et al. Long term survival data and prognostic factors of a complete response to chemotherapy in patients with head and neck cancer treated with platinum-based induction chemotherapy: A Hellenic Co-operative Oncology Group study. Med Pediatr Oncol. 1997;28:401–410. - PubMed
-
- Do KA, Johnson MM, Doherty DA, et al. Second primary tumors in patients with upper aerodigestive tract cancers: Joint effects of smoking and alcohol (United States) Cancer Causes Control. 2003;14:131–138. - PubMed
-
- Khuri FR, Lee JJ, Lippman SM, et al. Randomized phase III trial of low-dose isotretinoin for prevention of second primary tumors in stage I and II head and neck cancer patients. J Natl Cancer Inst. 2006;98:441–450. - PubMed
-
- Meyer F, Bairati I, Fortin A, et al. Interaction between antioxidant vitamin supplementation and cigarette smoking during radiation therapy in relation to long-term effects on recurrence and mortality: A randomized trial among head and neck cancer patients. Int J Cancer. 2008;122:1679–1683. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
