

Cost-effectiveness of a multicondition collaborative care intervention: a randomized controlled trial
- PMID: 22566583
- PMCID: PMC3840955
- DOI: 10.1001/archgenpsychiatry.2011.1548
Cost-effectiveness of a multicondition collaborative care intervention: a randomized controlled trial
Abstract
Context: Patients with depression and poorly controlled diabetes mellitus, coronary heart disease (CHD), or both have higher medical complication rates and higher health care costs, suggesting that more effective care management of psychiatric and medical disease control might also reduce medical service use and enhance quality of life.
Objective: To evaluate the cost-effectiveness of a multicondition collaborative treatment program (TEAMcare) compared with usual primary care (UC) in outpatients with depression and poorly controlled diabetes or CHD.
Design: Randomized controlled trial of a systematic care management program aimed at improving depression scores and hemoglobin A(1c) (HbA(1c)), systolic blood pressure (SBP), and low-density lipoprotein cholesterol (LDL-C) levels.
Setting: Fourteen primary care clinics of an integrated health care system.
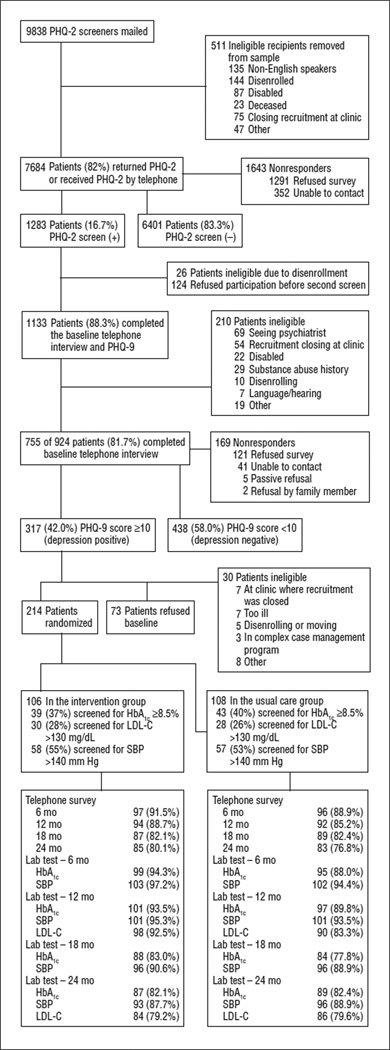
Patients: Population-based screening identified 214 adults with depressive disorder and poorly controlled diabetes or CHD.
Intervention: Physician-supervised nurses collaborated with primary care physicians to provide treatment of multiple disease risk factors.
Main outcome measures: Blinded assessments evaluated depressive symptoms, SBP, and HbA(1c) at baseline and at 6, 12, 18, and 24 months. Fasting LDL-C concentration was assessed at baseline and at 12 and 24 months. Health plan accounting records were used to assess medical service costs. Quality-adjusted life-years (QALYs) were assessed using a previously developed regression model based on intervention vs UC differences in HbA(1c), LDL-C, and SBP levels over 24 months.
Results: Over 24 months, compared with UC controls, intervention patients had a mean of 114 (95% CI, 79 to 149) additional depression-free days and an estimated 0.335 (95% CI, -0.18 to 0.85) additional QALYs. Intervention patients also had lower mean outpatient health costs of $594 per patient (95% CI, -$3241 to $2053) relative to UC patients.
Conclusions: For adults with depression and poorly controlled diabetes, CHD, or both, a systematic intervention program aimed at improving depression scores and HbA(1c), SBP, and LDL-C levels seemed to be a high-value program that for no or modest additional cost markedly improved QALYs.
Trial registration: clinicaltrials.gov Identifier: NCT00468676
Figures
References
-
- Wolff JL, Starfield B, Anderson G. Prevalence, expenditures, and complications of multiple chronic conditions in the elderly. Arch Intern Med. 2002;162(20):2269–2276. - PubMed
-
- Warshaw G. Introduction advances and challenges in care of older people with chronic illness. Generation. 2006;30(3):5–10.
-
- Anderson G, Horvath J. Chronic Conditions: Making the Case for Ongoing Care: Robert Wood Johnson Foundation’s Partnership for Solutions. Baltimore, MD: Johns Hopkins University; 2002.
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
