

Fluorodeoxyglucose positron emission tomography in anti-N-methyl-D-aspartate receptor encephalitis: distinct pattern of disease
- PMID: 22566598
- PMCID: PMC3740122
- DOI: 10.1136/jnnp-2011-301969
Fluorodeoxyglucose positron emission tomography in anti-N-methyl-D-aspartate receptor encephalitis: distinct pattern of disease
Abstract
Background: Patients with encephalitis associated with antibodies against N-methyl-D-aspartate-receptor antibody (NMDAR-ab) encephalitis frequently show psychotic symptoms, amnesia, seizures and movement disorders. While brain MRI in NMDAR-ab encephalitis is often normal, abnormalities of cerebral glucose metabolism have been demonstrated by positron emission tomography (PET) with 18F-fluorodeoxyglucose(FDG) in a few usually isolated case reports. However, a common pattern of FDG-PET abnormalities has not been reported.
Methods: The authors retrospectively identified six patients with NMDAR-ab encephalitis in two large German centres who underwent at least one whole-body FDG-PET for tumour screening between January 2007 and July 2010. They analysed the pattern of cerebral uptake derived from whole-body PET data for characteristic changes of glucose metabolism compared with controls, and the changes of this pattern during the course of the disease.
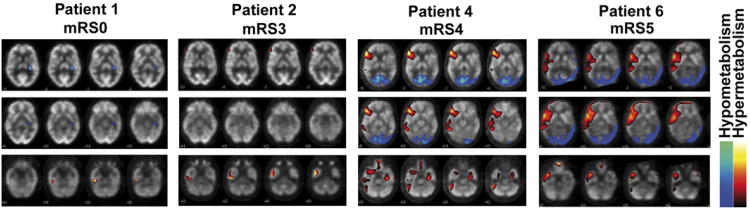
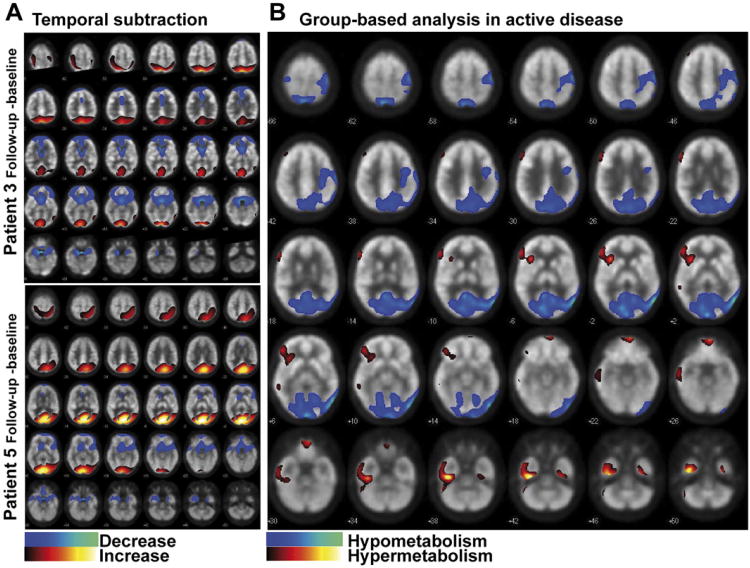
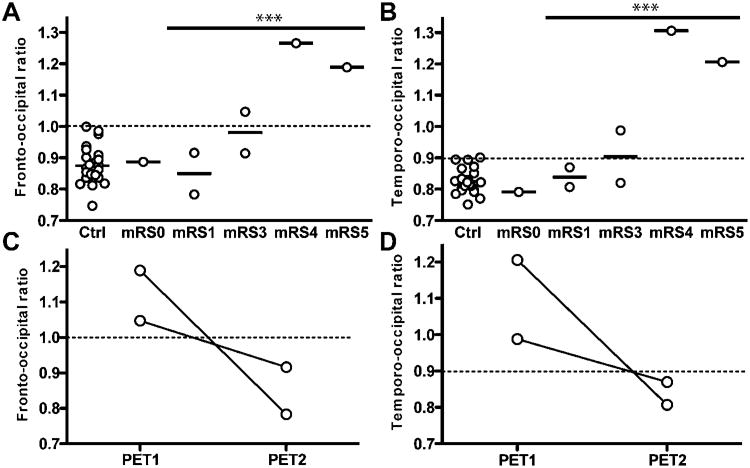
Results: Groupwise analysis revealed that patients with NMDAR-ab encephalitis showed relative frontal and temporal glucose hypermetabolism associated with occipital hypometabolism. Cross-sectional analysis of the group demonstrated that the extent of these changes is positively associated with clinical disease severity. Longitudinal analysis of two cases showed normalisation of the pattern of cerebral glucose metabolism with recovery.
Conclusions: A characteristic change in cerebral glucose metabolism during NMDAR-ab encephalitis is an increased frontotemporal-to-occipital gradient. This pattern correlates with disease severity. Similar changes have been observed in psychosis induced by NMDAR antagonists. Thus, this pattern might be a consequence of impaired NMDAR function.
Conflict of interest statement
Figures
References
-
- Prüss H, Dalmau J, Harms L, et al. Retrospective analysis of NMDA receptor antibodies in encephalitis of unknown origin. Neurology. 2010;75:1735–9. - PubMed
-
- Granerod J, Ambrose HE, Davies NW, et al. UK Health Protection Agency (HPA) Aetiology of Encephalitis Study Group. Causes of encephalitis and differences in their clinical presentations in England: a multicentre, population-based prospective study. Lancet Infect Dis. 2010;10:835–44. - PubMed
-
- Maeder-Ingvar M, Prior JO, Irani SR, et al. FDG-PET hyperactivity in basal ganglia correlating with clinical course in anti-NDMA-R antibodies encephalitis. J Neurol Neurosurg Psychiatry. 2010;32:235–6. - PubMed
-
- Mohr BC, Minoshima S. F-18 fluorodeoxyglucose PET/CT findings in a case of anti-NMDA receptor encephalitis. Clin Nucl Med. 2010;35:461–3. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources