

The effect of a biofeedback-based stress management tool on physician stress: a randomized controlled clinical trial
- PMID: 22567069
- PMCID: PMC3345375
The effect of a biofeedback-based stress management tool on physician stress: a randomized controlled clinical trial
Abstract
Background: Physicians often experience work-related stress that may lead to personal harm and impaired professional performance. Biofeedback has been used to manage stress in various populations.
Objective: To determine whether a biofeedback-based stress management tool, consisting of rhythmic breathing, actively self-generated positive emotions and a portable biofeedback device, reduces physician stress.
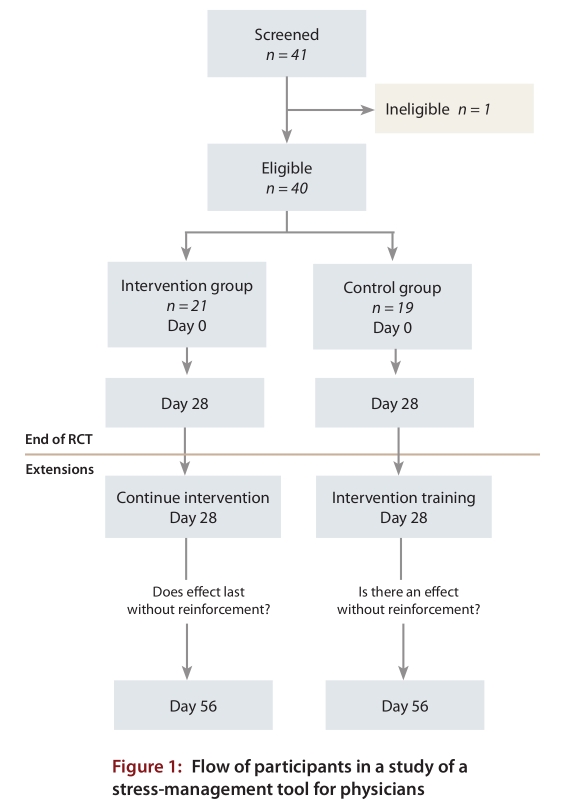
Design: Randomized controlled trial measuring efficacy of a stress-reduction intervention over 28 days, with a 28-day open-label trial extension to assess effectiveness.
Setting: Urban tertiary care hospital.
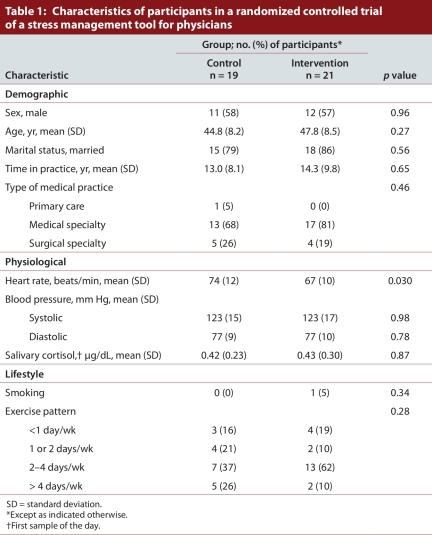
Participants: Forty staff physicians (23 men and 17 women) from various medical practices (1 from primary care, 30 from a medical specialty and 9 from a surgical specialty) were recruited by means of electronic mail, regular mail and posters placed in the physicians' lounge and throughout the hospital.
Intervention: Physicians in the intervention group were instructed to use a biofeedback-based stress management tool three times daily. Participants in both the control and intervention groups received twice-weekly support visits from the research team over 28 days, with the intervention group also receiving re-inforcement in the use of the stress management tool during these support visits. During the 28-day extension period, both the control and the intervention groups received the intervention, but without intensive support from the research team.
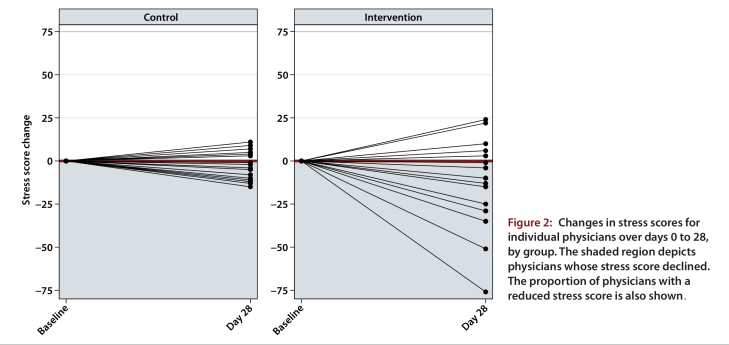
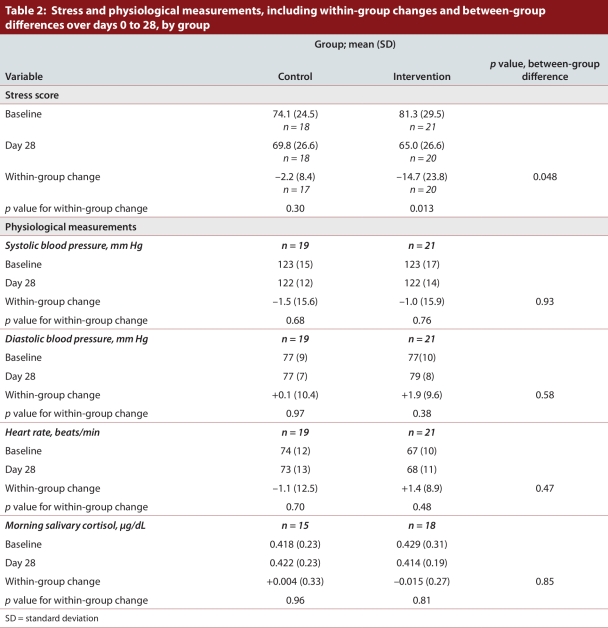
Main outcome measure: Stress was measured with a scale developed to capture short-term changes in global perceptions of stress for physicians (maximum score 200).
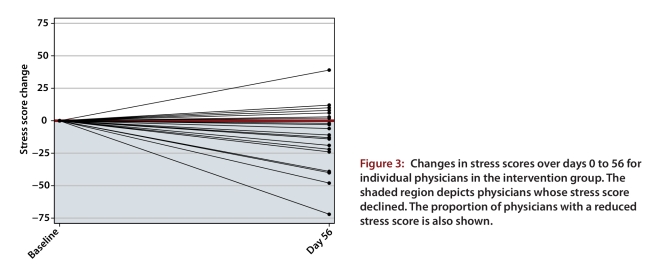
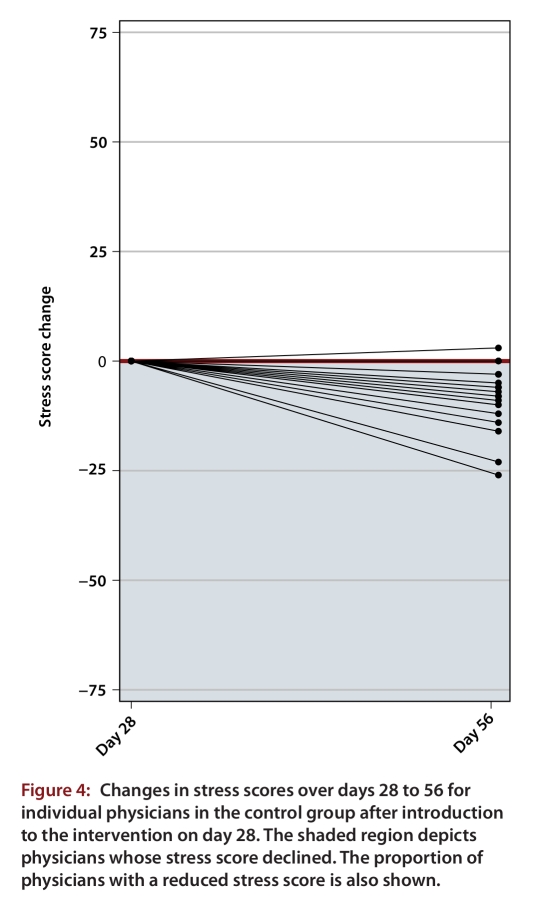
Results: During the randomized controlled trial (days 0 to 28), the mean stress score declined significantly for the intervention group (change -14.7, standard deviation [SD] 23.8; p = 0.013) but not for the control group (change -2.2, SD 8.4; p = 0.30). The difference in mean score change between the groups was 12.5 (p = 0.048). The lower mean stress scores in the intervention group were maintained during the trial extension to day 56. The mean stress score for the control group changed significantly during the 28-day extension period (change -8.5, SD 7.6; p < 0.001).
Conclusion: A biofeedback-based stress management tool may be a simple and effective stress-reduction strategy for physicians.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Arnetz Bengt B. Psychosocial challenges facing physicians of today. Soc Sci Med. 2001;52(2):203–213. doi: 10.1016/S0277-9536(00)00220-3. http://linkinghub.elsevier.com/retrieve/pii/S0277953600002203 - DOI - PubMed
-
- Wallace Jean E, Lemaire Jane B, Ghali William A. Physician wellness: a missing quality indicator. Lancet. 2009;374(9702):1714–1721. doi: 10.1016/S0140-6736(09)61424-0. http://linkinghub.elsevier.com/retrieve/pii/S0140673609614240 - DOI - PubMed
-
- Holroyd Kenneth A, Penzien Donald B. Pharmacological versus non-pharmacological prophylaxis of recurrent migraine headache: a meta-analytic review of clinical trials. Pain. 1990;42(1):1–13. doi: 10.1016/0304-3959(90)91085-W. http://linkinghub.elsevier.com/retrieve/pii/030439599091085W - DOI - PubMed
-
- Kirsch Cynthia A, Blanchard Edward B, Parnes Steven M. A multiple-baseline evaluation of the treatment of subjective tinnitus with relaxation training and biofeedback. Biofeedback Self Regul. 1987;12(4):295–312. doi: 10.1007/BF00998721. http://www.springerlink.com/index/10.1007/BF00998721 - DOI - PubMed
-
- Goldstein I B, Shapiro D, Thananopavaran C. Home relaxation techniques for essential hypertension. Psychosom Med. 1984;46(5):398–414. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical