

Re-irradiation: outcome, cumulative dose and toxicity in patients retreated with stereotactic radiotherapy in the abdominal or pelvic region
- PMID: 22568625
- PMCID: PMC4527454
- DOI: 10.7785/tcrt.2012.500261
Re-irradiation: outcome, cumulative dose and toxicity in patients retreated with stereotactic radiotherapy in the abdominal or pelvic region
Abstract
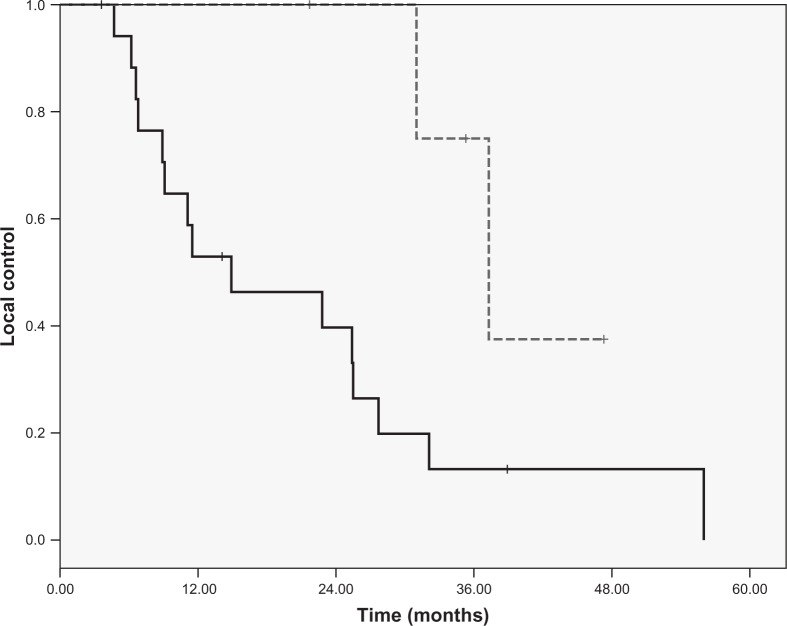
The purpose of the present study was to explore the outcome, cumulative dose in tumor and organs at risk and toxicity after extra-cranial stereotactic re-irradiation. Twenty-seven patients were evaluated who had been re-irradiated with stereotactic body radiotherapy (SBRT) after conventional radiotherapy (CRT). The dose summation of the SBRT and CRT plans was done by dose point calculations accounting for fraction size by the linear-quadratic model. Efficacy and toxicity was scored by looking at the reduction in tumor size, pain and bleeding. Symptomatic response was observed in 96% of the patients. The median maximum SBRT dose to the tumor was 90 Gy(3) (range: 42-420 Gy(3)). The median cumulative dose for the rectum, bowel and bladder resulted in 104 Gy(3), 98 Gy(3) and 113 Gy(3), respectively. No grades 5, 4 and 3 acute and late toxicity was observed.
In conclusion: re-irradiation to the same region using extra-cranial stereotactic radiotherapy is feasible and resulted in a 96% symptomatic response with low toxicity.
Conflict of interest statement
Figures
References
-
- Rades D., Rudat V., Veninga T., Stalpers L. J., Hoskin P. J., Schild S. E. Prognostic factors for functional outcome and survival after reirradiation for in-field recurrences of metastatic spinal cord compression. Cancer 11, 1090–1096 (2008). - PubMed
-
- Nieder C., Grosu A. L., Andratschke N. H., Molls M. Update of human spinal cord reirradiation tolerance based on additional data from 38 patients. Int J Radiat Oncol Biol Phys 66, 1446–1449 (2006). - PubMed
-
- Morris D. E. Clinical experience with retreatment for palliation. Semin Radiat Oncol 10, 210–221 (2000). - PubMed
-
- Nieder C., Grosu A. L., Andratschke N. H., Molls M. Proposal of human spinal cord reirradiation dose based on collection of data from 40 patients. Int J Radiat Oncol Biol Phys 61, 851–855 (2005). - PubMed
-
- Stewart F. A., van der Kogel A. J. Retreatment Tolerance of Normal Tissues. Semin Radiat Oncol 4, 103–111 (1994). - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
