

Improving blood pressure control through a clinical pharmacist outreach program in patients with diabetes mellitus in 2 high-performing health systems: the adherence and intensification of medications cluster randomized, controlled pragmatic trial
- PMID: 22570370
- PMCID: PMC3999872
- DOI: 10.1161/CIRCULATIONAHA.111.089169
Improving blood pressure control through a clinical pharmacist outreach program in patients with diabetes mellitus in 2 high-performing health systems: the adherence and intensification of medications cluster randomized, controlled pragmatic trial
Abstract
Background: Even in high-performing health systems, some patients with diabetes mellitus have poor blood pressure (BP) control because of poor medication adherence and lack of medication intensification. We examined whether the Adherence and Intensification of Medications intervention, a pharmacist-led intervention combining elements found in efficacy studies to lower BP, improved BP among patients with diabetes mellitus with persistent hypertension and poor refill adherence or insufficient medication intensification in 2 high-performing health systems.
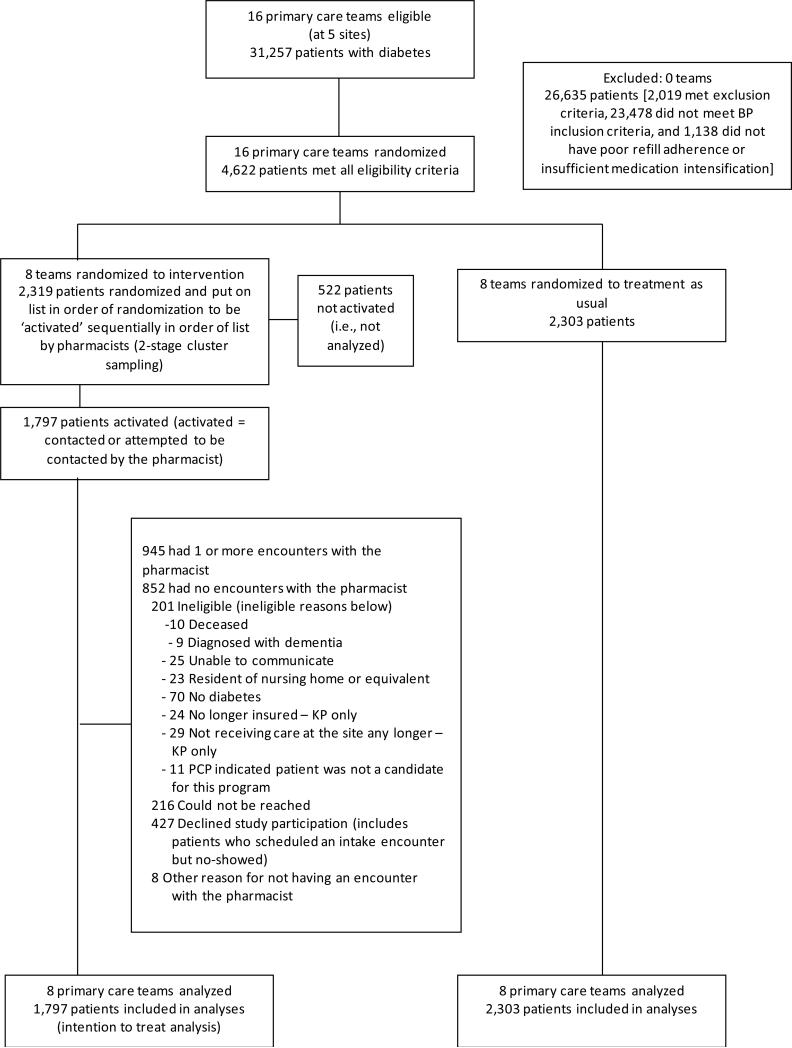
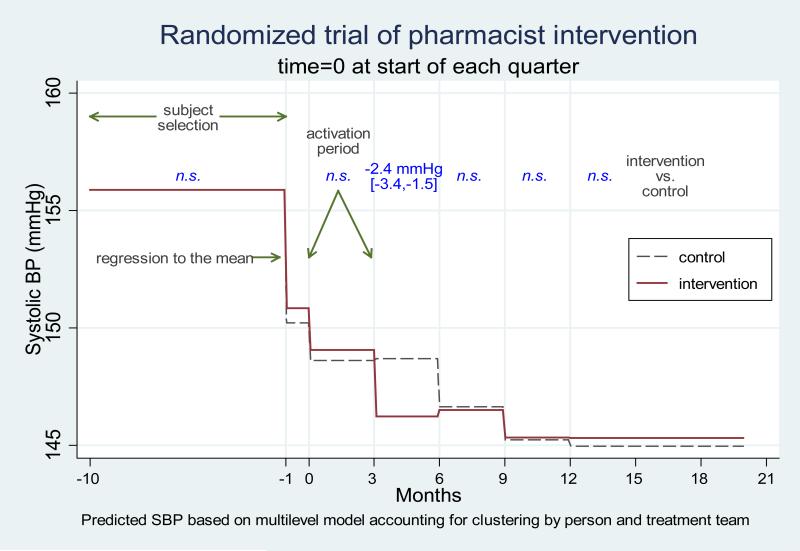
Methods and results: We conducted a prospective, multisite cluster randomized pragmatic trial with randomization of 16 primary care teams at 5 medical centers (3 Veterans Affairs and 2 Kaiser Permanente) to the Adherence and Intensification of Medications intervention or usual care. The primary outcome was relative change in systolic BP (SBP), comparing 1797 intervention with 2303 control team patients, from 6 months preceding to 6 months after the 14-month intervention period. We examined shorter-term changes in SBP as a secondary outcome. The mean SBP decrease from 6 months before to 6 months after the intervention period was ≈9 mm Hg in both arms. Mean SBPs of eligible intervention patients were 2.4 mm Hg lower (95% CI: -3.4 to -1.5; P<0.001) immediately after the intervention than those achieved by control patients.
Conclusions: The Adherence and Intensification of Medications program more rapidly lowered SBPs among intervention patients, but usual-care patients achieved equally low SBP levels by 6 months after the intervention period. These findings show the importance of evaluating in different real-life clinical settings programs found in efficacy trials to be effective before urging their widespread adoption in all settings.
Clinical trial registration: URL: http://clinicaltrials.gov. Unique identifier: NCT00495794.
Figures
Comment in
-
Taking AIM at a moving target: the challenge of improving on high-performance care.Circulation. 2012 Jun 12;125(23):2812-4. doi: 10.1161/CIRCULATIONAHA.112.110783. Epub 2012 May 8. Circulation. 2012. PMID: 22570369 No abstract available.
References
-
- The CDC Diabetes Cost-effectiveness Group Cost-effectiveness of intensive glycemic control, intensified hypertension control, and serum cholesterol level reduction for type 2 diabetes. JAMA. 2002;287(19):2542–2551. - PubMed
-
- Zhang P, Engelgau MM, Norris SL, Gregg EW, Narayan KM. Application of economic analysis to diabetes and diabetes care. Ann Intern Med. 2004;140(11):972–977. - PubMed
-
- Egan BM, Zhao Y, Axon RN. US trends in prevalence, awareness, treatment, and control of hypertension, 1988-2008. JAMA. 2010;303(20):2043–2050. - PubMed
