

Management of focal chondral lesion in the knee joint
- PMID: 22570833
- PMCID: PMC3341803
- DOI: 10.5792/ksrr.2011.23.4.185
Management of focal chondral lesion in the knee joint
Abstract
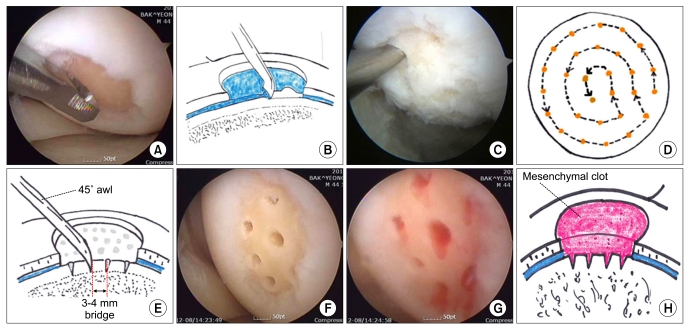
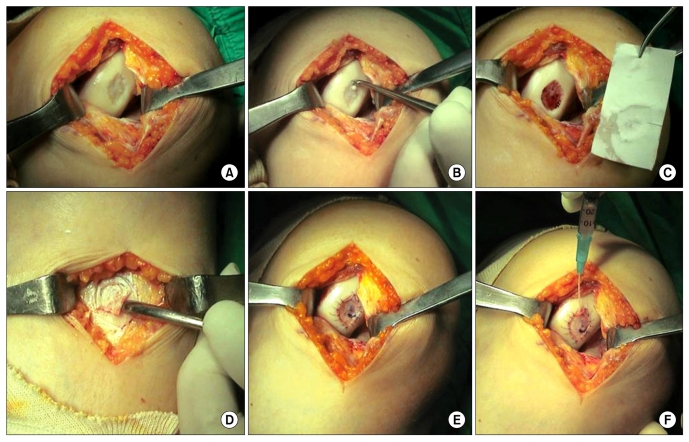
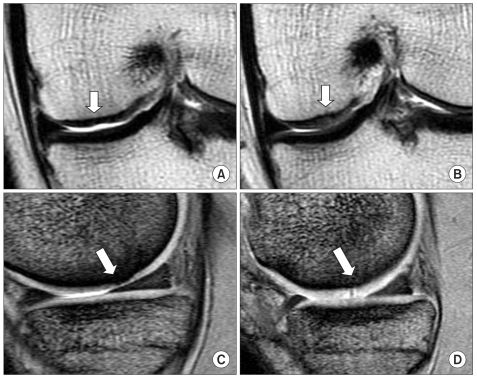
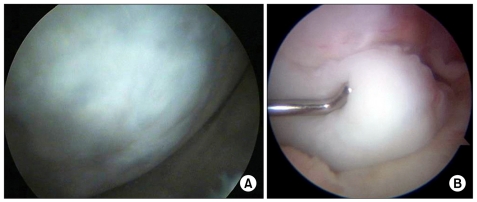
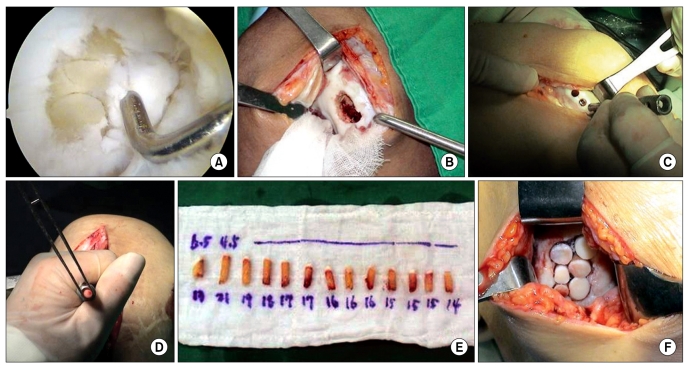
Articular cartilage does not contain vascular, nervous and lymphatic tissue and chondrocytes hardly participate in the healing or repair process of chondral tissue because of being surrounded by plenty of extracellular matrix. Therefore, the injury to articular cartilage frequently requires an operative treatment. The goal of surgical repair of articular cartilage is to regenerate nearly normal chondral tissue and prevent degenerative arthritis caused by the articular cartilage defect. Microfracture is a kind of cartilage repair procedure that makes a fibrin clot containing mesenchymal stem cells in the chondral lesion. Microfracture is a simple procedure but it has a disadvantage that the repaired tissue is fibrocartilage. Autologous chondrocyte implantation has an advantage that it implants fully differentiated chondrocytes to the lesion, which theoretically produces hyaline cartilage. Its disadvantages are that it is a two stage and a costly procedure. Osteochondral autograft transplantation is a one stage procedure and repairs the lesion with hyaline cartilage. But its limitation is the lack of donor site availability. Surgeons who understand the theoretical background, indications, surgical methods, rehabilitation, complications, and clinical course of cartilage repair procedures can achieve the goal of preventing degenerative arthritis.
Keywords: Articular cartilage; Focal chondral lesion; Knee joint; Management.
Figures
References
-
- Buckwalter JA, Mankin HJ. Articular cartilage. Part II: degeneration and osteoarthrosis, repair, regeneration, and transplantation. J Bone Joint Surg Am. 1997;79:612–632.
-
- Shah MR, Kaplan KM, Meislin RJ, Bosco JA., 3rd Articular cartilage restoration of the knee. Bull NYU Hosp Jt Dis. 2007;65:51–60. - PubMed
-
- Curl WW, Krome J, Gordon ES, Rushing J, Smith BP, Poehling GG. Cartilage injuries: a review of 31,516 knee arthroscopies. Arthroscopy. 1997;13:456–460. - PubMed
-
- Craig W, David JW, Ming HZ. A current review on the biology and treatment of the articular cartilage defects (part I & part II) J Musculoskelet Res. 2003;7:157–181.
-
- Messner K, Maletius W. The long-term prognosis for severe damage to weight-bearing cartilage in the knee: a 14-year clinical and radiographic follow-up in 28 young athletes. Acta Orthop Scand. 1996;67:165–168. - PubMed
LinkOut - more resources
Full Text Sources