

Lenalidomide after stem-cell transplantation for multiple myeloma
- PMID: 22571201
- PMCID: PMC3744390
- DOI: 10.1056/NEJMoa1114083
Lenalidomide after stem-cell transplantation for multiple myeloma
Abstract
Background: Data are lacking on whether lenalidomide maintenance therapy prolongs the time to disease progression after autologous hematopoietic stem-cell transplantation in patients with multiple myeloma.
Methods: Between April 2005 and July 2009, we randomly assigned 460 patients who were younger than 71 years of age and had stable disease or a marginal, partial, or complete response 100 days after undergoing stem-cell transplantation to lenalidomide or placebo, which was administered until disease progression. The starting dose of lenalidomide was 10 mg per day (range, 5 to 15).
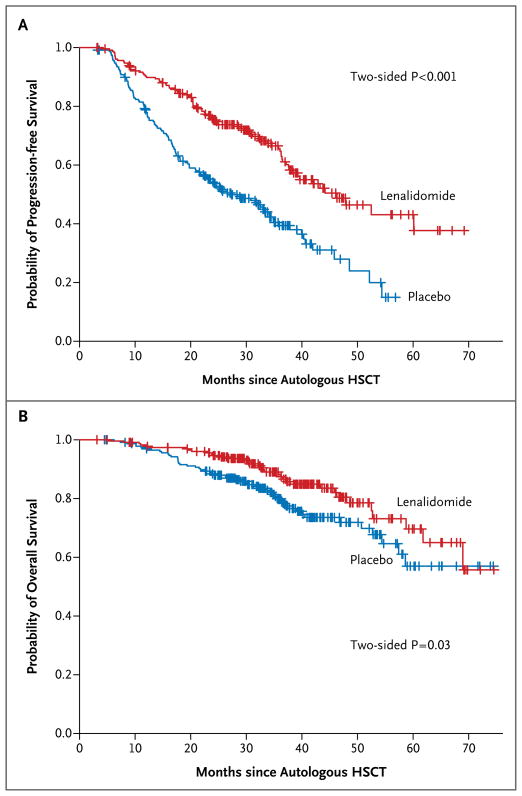
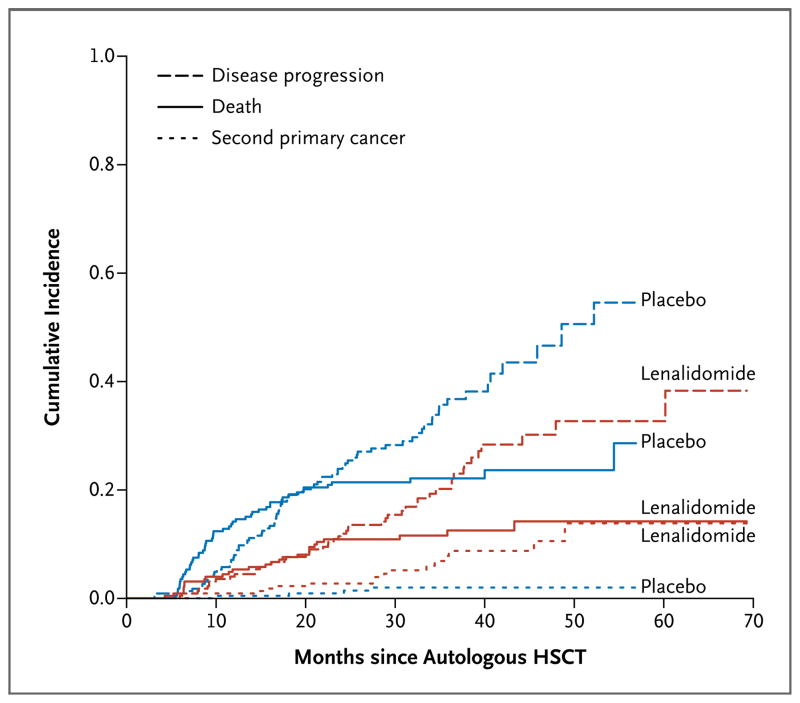
Results: The study-drug assignments were unblinded in 2009, when a planned interim analysis showed a significantly longer time to disease progression in the lenalidomide group. At unblinding, 20% of patients who received lenalidomide and 44% of patients who received placebo had progressive disease or had died (P<0.001); of the remaining 128 patients who received placebo and who did not have progressive disease, 86 crossed over to lenalidomide. At a median follow-up of 34 months, 86 of 231 patients who received lenalidomide (37%) and 132 of 229 patients who received placebo (58%) had disease progression or had died. The median time to progression was 46 months in the lenalidomide group and 27 months in the placebo group (P<0.001). A total of 35 patients who received lenalidomide (15%) and 53 patients who received placebo (23%) died (P=0.03). More grade 3 or 4 hematologic adverse events and grade 3 nonhematologic adverse events occurred in patients who received lenalidomide (P<0.001 for both comparisons). Second primary cancers occurred in 18 patients who received lenalidomide (8%) and 6 patients who received placebo (3%).
Conclusions: Lenalidomide maintenance therapy, initiated at day 100 after hematopoietic stem-cell transplantation, was associated with more toxicity and second cancers but a significantly longer time to disease progression and significantly improved overall survival among patients with myeloma. (Funded by the National Cancer Institute; ClinicalTrials.gov number, NCT00114101.).
Figures
Comment in
-
Lenalidomide in myeloma--a high-maintenance friend.N Engl J Med. 2012 May 10;366(19):1836-8. doi: 10.1056/NEJMe1202819. N Engl J Med. 2012. PMID: 22571206 No abstract available.
-
Lenalidomide for multiple myeloma.N Engl J Med. 2012 Aug 9;367(6):573; author reply 573-5. doi: 10.1056/NEJMc1206734. N Engl J Med. 2012. PMID: 22873542 No abstract available.
-
[New treatment strategies for multiple myeloma].Internist (Berl). 2013 Jul;54(7):892-6. doi: 10.1007/s00108-013-3299-3. Internist (Berl). 2013. PMID: 23748490 German. No abstract available.
References
-
- Stewart AK, Richardson PG, San-Miguel JF. How I treat multiple myeloma in younger patients. Blood. 2009;114:5436–43. [Erratum, Blood 2010;115:4006.] - PubMed
-
- Palumbo A, Anderson K. Multiple myeloma. N Engl J Med. 2011;364:1046–60. - PubMed
-
- Southwest Oncology Group Study. Remission maintenance therapy for multiple myeloma. Arch Intern Med. 1975;135:147–52. - PubMed
-
- Fritz E, Ludwig H. Interferon-alpha treatment in multiple myeloma: meta-analysis of 30 randomised trials among 3948 patients. Ann Oncol. 2000;11:1427–36. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- U10 HL069294/HL/NHLBI NIH HHS/United States
- U10 HL109526/HL/NHLBI NIH HHS/United States
- UG1 HL069286/HL/NHLBI NIH HHS/United States
- U10 HL069290/HL/NHLBI NIH HHS/United States
- UG1 HL069315/HL/NHLBI NIH HHS/United States
- U10 HL069330/HL/NHLBI NIH HHS/United States
- U10 HL069334/HL/NHLBI NIH HHS/United States
- U01 HL069294/HL/NHLBI NIH HHS/United States
- P50 CA100707/CA/NCI NIH HHS/United States
- U10 HL069315/HL/NHLBI NIH HHS/United States
- U10 HL069348/HL/NHLBI NIH HHS/United States
- U24 CA076518/CA/NCI NIH HHS/United States
- U10 CA021115/CA/NCI NIH HHS/United States
- U10 HL069286/HL/NHLBI NIH HHS/United States
- U10 CA031946/CA/NCI NIH HHS/United States
- U10 CA033601/CA/NCI NIH HHS/United States
- U10 HL069301/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous