

The predictive value of histological tumor regression grading (TRG) for therapeutic evaluation in locally advanced esophageal carcinoma treated with neoadjuvant chemotherapy
- PMID: 22572013
- PMCID: PMC3777510
- DOI: 10.5732/cjc.011.10406
The predictive value of histological tumor regression grading (TRG) for therapeutic evaluation in locally advanced esophageal carcinoma treated with neoadjuvant chemotherapy
Abstract
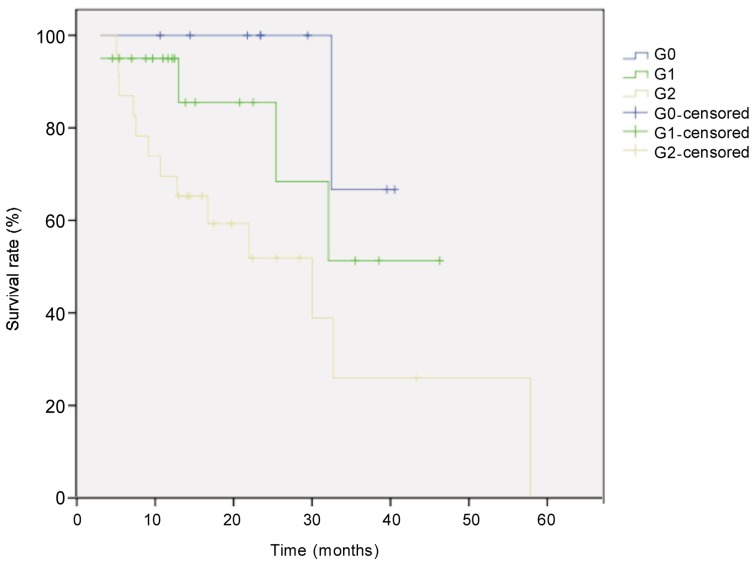
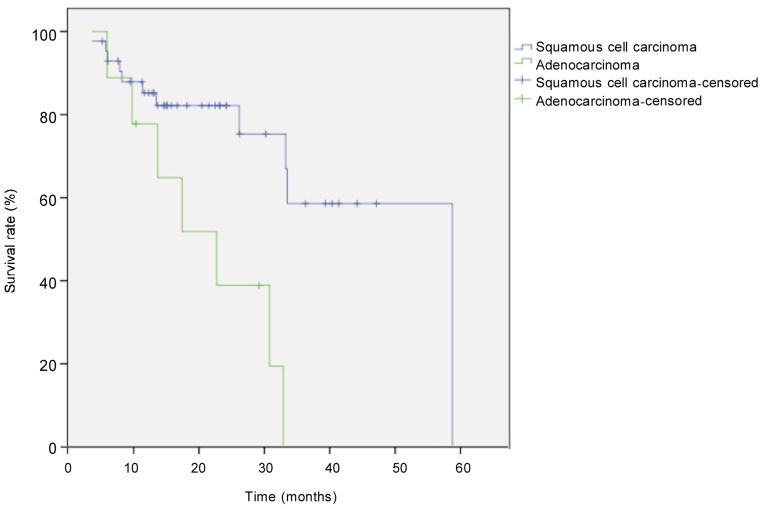
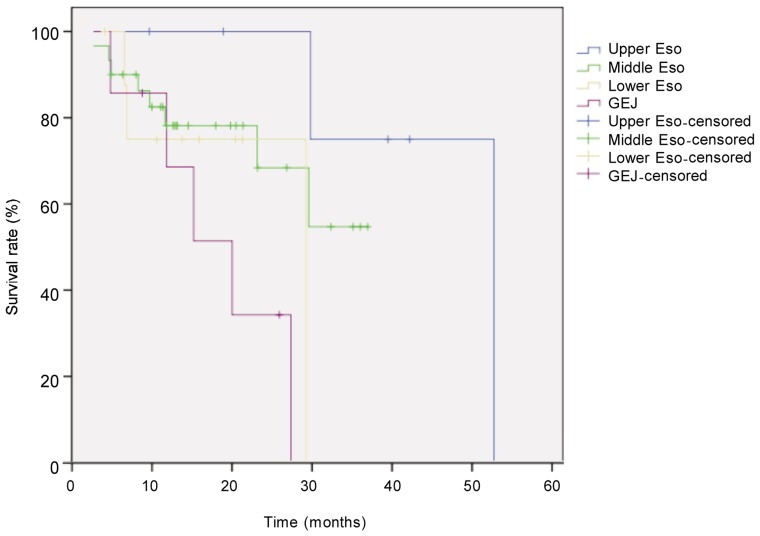
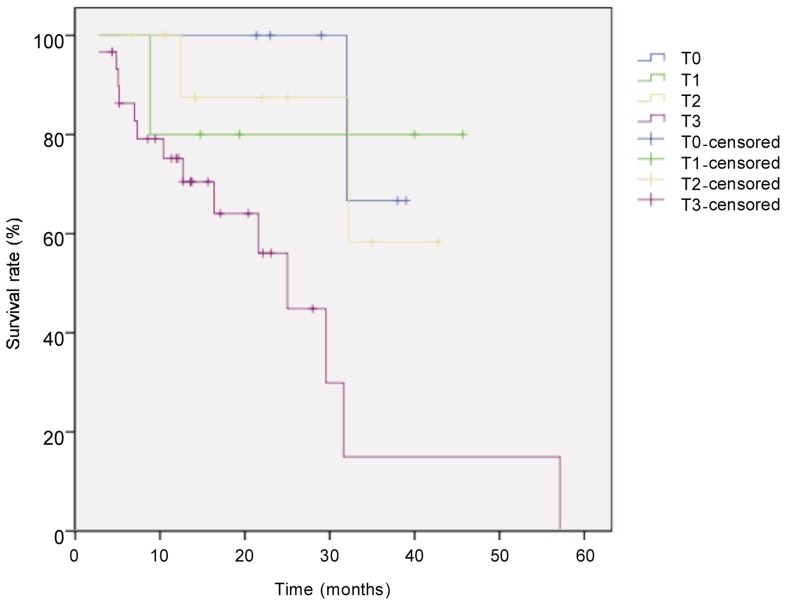
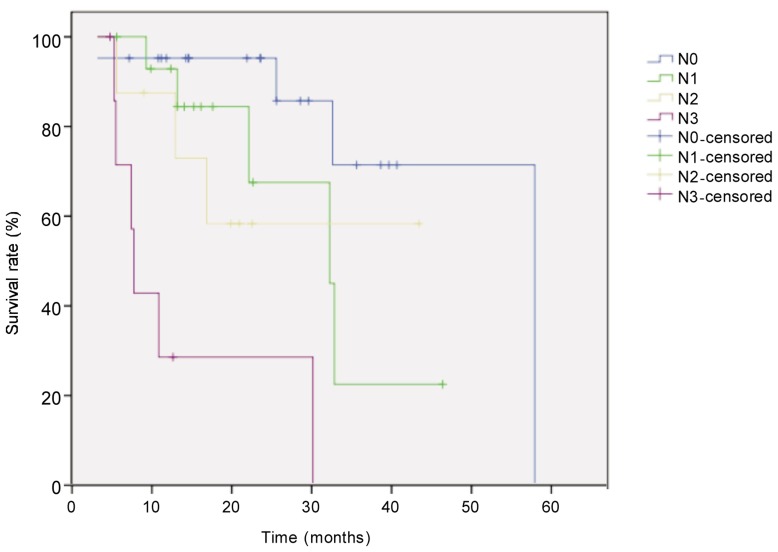
Response criteria remain controversial in therapeutic evaluation for locally advanced esophageal carcinoma treated with neoadjuvant chemotherapy. We aimed to identify the predictive value of tumor regression grading (TRG) in tumor response and prognosis. Fifty-two patients who underwent neoadjuvant chemotherapy followed by esophagectomy and radical 2-field lymphadenectomy between June 2007 and June 2011 were included in this study. All tissue specimens were reassessed according to the TRG scale. Potential prognostic factors, including clinicopathologic factors, were evaluated. Survival curves were generated by using the Kaplan-Meier method and compared with the log-rank test. Prognostic factors were determined with multivariate analysis by using the Cox regression model. Our results showed that of 52 cases, 43 (83%) were squamous cell carcinoma and 9 (17%) were adenocarcinoma. TRG was correlated with pathologic T(P = 0.006) and N (P < 0.001) categories. Median overall survival for the entire cohort was 33 months. The 1- and 2-year overall survival rates were 71% and 44%, respectively. Univariate survival analysis results showed that favorable prognostic factors were histological subtype (P = 0.003), pathologic T category (P = 0.026), pathologic N category (P < 0.001), and TRG G0 (P = 0.041). Multivariate analyses identified pathologic N category (P < 0.001) as a significant independent prognostic parameter. Our results indicate that histomorphologic TRG can be considered as an alternative option to predict the therapeutic efficacy and prognostic factor for patients with locally advanced esophageal carcinoma treated by neoadjuvant chemotherapy.
Figures
Similar articles
-
Comparison of five tumor regression grading systems for gastric adenocarcinoma after neoadjuvant chemotherapy: a retrospective study of 192 cases from National Cancer Center in China.BMC Gastroenterol. 2017 Mar 14;17(1):41. doi: 10.1186/s12876-017-0598-5. BMC Gastroenterol. 2017. PMID: 28292272 Free PMC article.
-
Long-term results of a phase II trial of neoadjuvant chemotherapy followed by esophagectomy for locally advanced esophageal neoplasm.Ann Thorac Surg. 2008 Jun;85(6):1930-6; discussion 1936-7. doi: 10.1016/j.athoracsur.2008.01.097. Ann Thorac Surg. 2008. PMID: 18498797 Clinical Trial.
-
Prognostic significance of tumor regression grade for patients with esophageal squamous cell carcinoma after neoadjuvant chemotherapy followed by surgery.J Surg Oncol. 2016 Mar;113(4):390-6. doi: 10.1002/jso.24151. Epub 2016 Jan 12. J Surg Oncol. 2016. PMID: 27100024
-
Prognostic nomogram for previously untreated patients with esophageal squamous cell carcinoma after esophagectomy followed by adjuvant chemotherapy.Jpn J Clin Oncol. 2016 Apr;46(4):336-43. doi: 10.1093/jjco/hyv206. Epub 2016 Jan 26. Jpn J Clin Oncol. 2016. PMID: 26819278 Free PMC article.
-
Factors affecting postoperative course and survival after en bloc resection for esophageal carcinoma.Ann Thorac Surg. 2004 Oct;78(4):1177-83. doi: 10.1016/j.athoracsur.2004.02.068. Ann Thorac Surg. 2004. PMID: 15464466 Review.
Cited by
-
Investigating the susceptibility of treatment-resistant oesophageal tumours to natural killer cell-mediated responses.Clin Exp Med. 2023 Jun;23(2):411-425. doi: 10.1007/s10238-022-00811-6. Epub 2022 Apr 1. Clin Exp Med. 2023. PMID: 35364779 Free PMC article.
-
Comparison of tumor regression grading system in locally advanced esophageal squamous cell carcinoma after preoperative radio-chemotherapy to determine the most accurate system predicting prognosis.J Gastrointest Oncol. 2019 Apr;10(2):276-282. doi: 10.21037/jgo.2018.12.01. J Gastrointest Oncol. 2019. PMID: 31032095 Free PMC article.
-
Prognostic value of pathological lymph node status and primary tumour regression grading following neoadjuvant chemotherapy - results from the MRC OE02 oesophageal cancer trial.Histopathology. 2018 Jun;72(7):1180-1188. doi: 10.1111/his.13491. Epub 2018 Mar 25. Histopathology. 2018. PMID: 29465751 Free PMC article.
-
Nedaplatin concurrent with three-dimensional conformal radiotherapy for treatment of locally advanced esophageal carcinoma.World J Gastroenterol. 2013 Dec 28;19(48):9447-52. doi: 10.3748/wjg.v19.i48.9447. World J Gastroenterol. 2013. PMID: 24409075 Free PMC article. Clinical Trial.
-
Tumor regression grade in locally advanced rectal cancer after neoadjuvant chemoradiotherapy: influencing factors and prognostic significance.Int J Clin Exp Pathol. 2023 Jun 15;16(6):124-132. eCollection 2023. Int J Clin Exp Pathol. 2023. PMID: 37425225 Free PMC article.
References
-
- Rice TW, Blackstone EH, Rusch VW. 7th edition of the AJCC cancer staging manual: esophagus and esophagogastric junction. Ann Surg Oncol. 2010;17:1721–1724. - PubMed
-
- Refaely Y, Krasna MJ. Multimodality therapy for esophageal cancer. Surg Clin North Am. 2002;82:729–746. - PubMed
-
- Hyngstrom JR, Posner MC. Neoadjuvant strategies for the treatment of locally advanced esophageal cancer. J Surg Oncol. 2010;101:299–304. - PubMed
-
- Gao XS. Considerations of treatment standardization from the procession of NCCN guideline of esophageal cancer. Chin J Cancer. 2010;29:860–864. - PubMed
-
- Kim TJ, Kim HY, Lee KW, et al. et al. Multimodality assessment of esophageal cancer: preoperative staging and monitoring of response to therapy. Radiographics. 2009;29:403–421. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical