

Esophageal toxicity from high-dose, single-fraction paraspinal stereotactic radiosurgery
- PMID: 22572079
- PMCID: PMC3392527
- DOI: 10.1016/j.ijrobp.2012.01.080
Esophageal toxicity from high-dose, single-fraction paraspinal stereotactic radiosurgery
Abstract
Purpose: To report the esophageal toxicity from single-fraction paraspinal stereotactic radiosurgery (SRS) and identify dosimetric and clinical risk factors for toxicity.
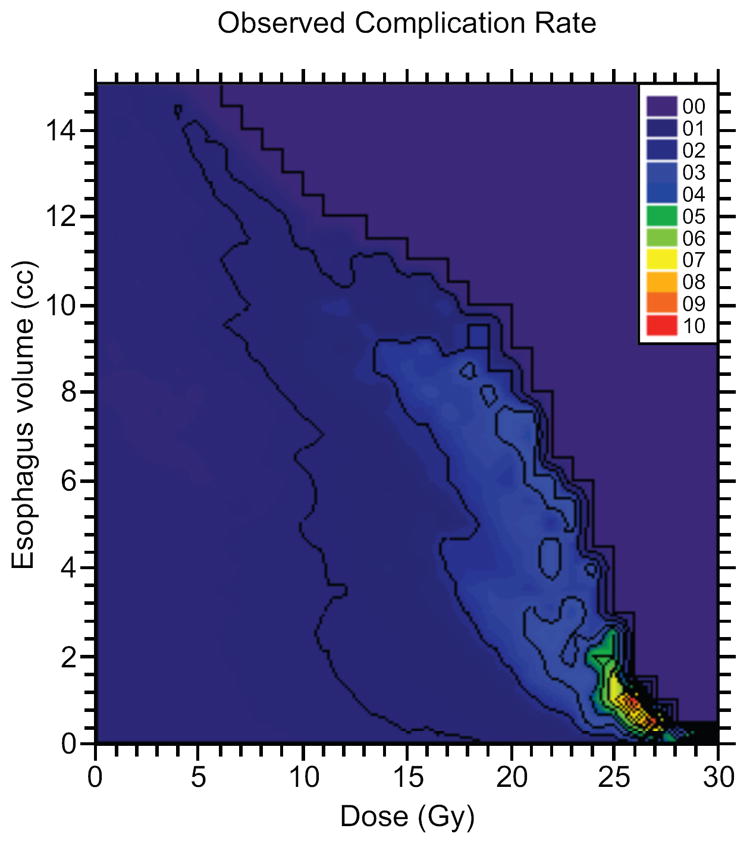
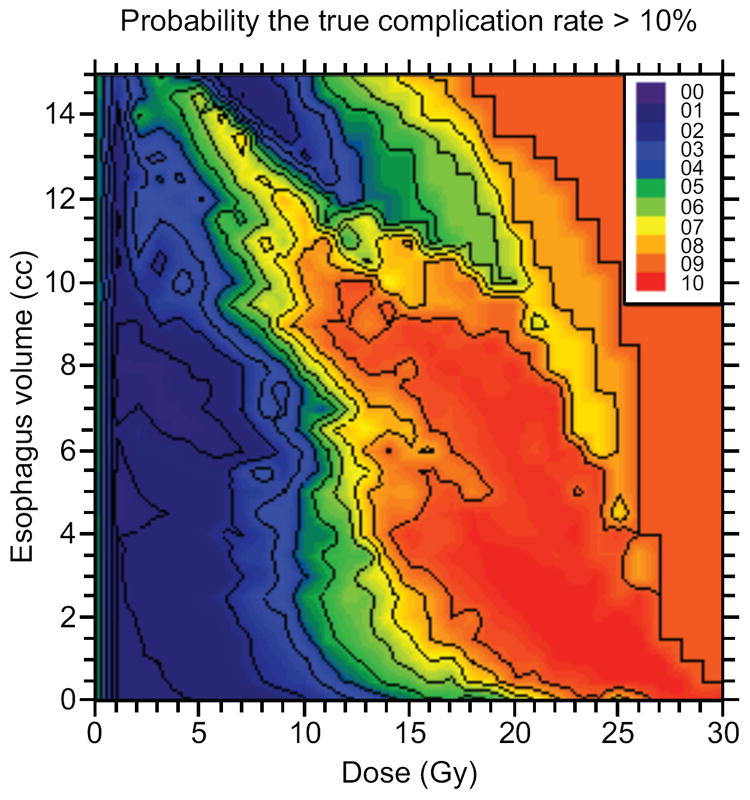
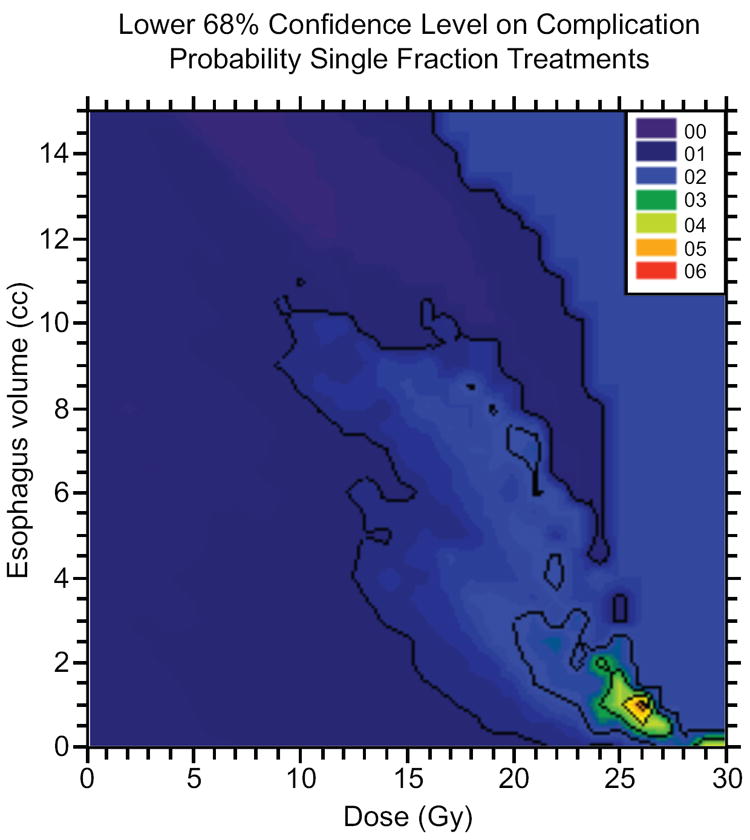
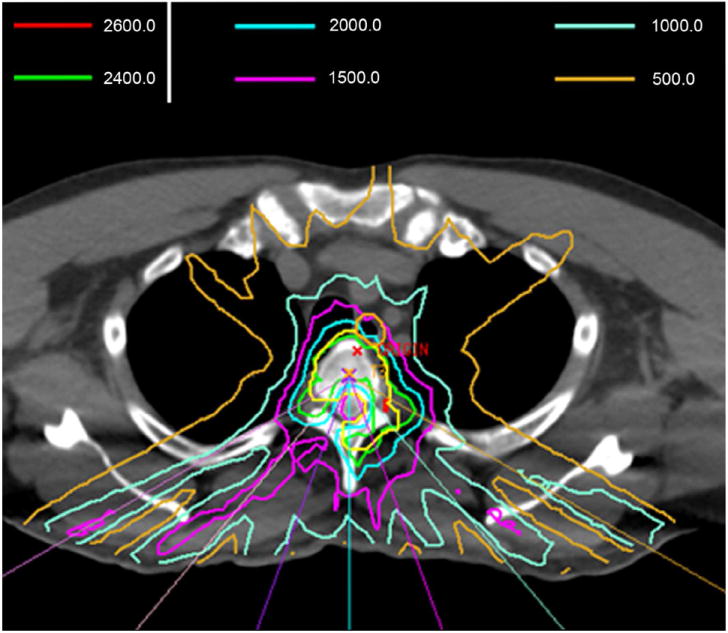
Methods and materials: A total of 204 spinal metastases abutting the esophagus (182 patients) were treated with high-dose single-fraction SRS during 2003-2010. Toxicity was scored using the National Cancer Institute Common Toxicity Criteria for Adverse Events, version 4.0. Dose-volume histograms were combined to generate a comprehensive atlas of complication incidence that identifies risk factors for toxicity. Correlation of dose-volume factors with esophageal toxicity was assessed using Fisher's exact test and logistic regression. Clinical factors were correlated with toxicity.
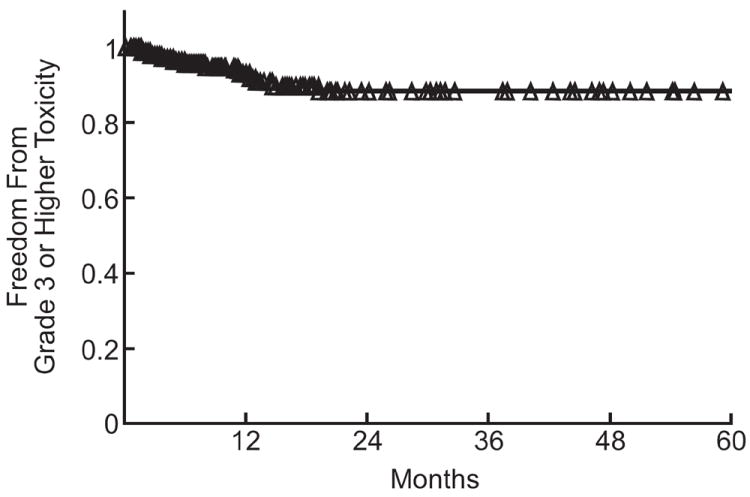
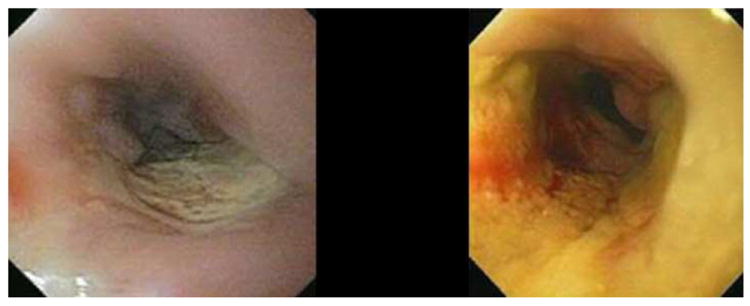
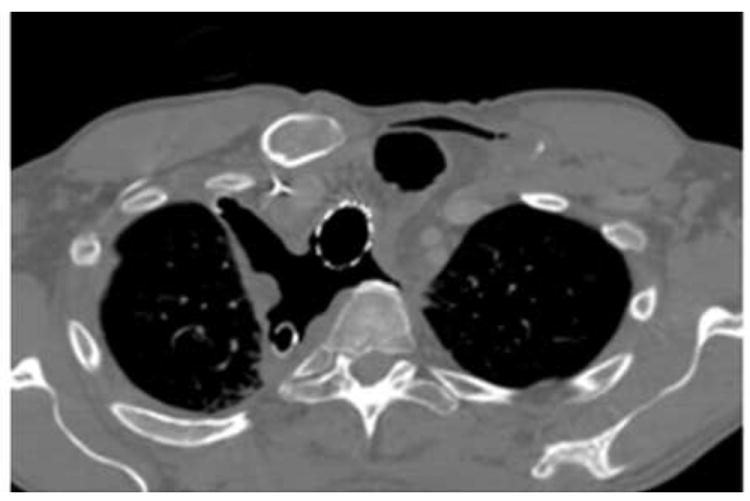
Results: The median dose to the planning treatment volume was 24 Gy. Median follow-up was 12 months (range, 3-81). There were 31 (15%) acute and 24 (12%) late esophageal toxicities. The rate of grade ≥3 acute or late toxicity was 6.8% (14 patients). Fisher's exact test resulted in significant median splits for grade ≥3 toxicity at V12 = 3.78 cm(3) (relative risk [RR] 3.7, P=.05), V15 = 1.87 cm(3) (RR 13, P=.0013), V20 = 0.11 cm(3) (RR 6, P=0.01), and V22 = 0.0 cm(3) (RR 13, P=.0013). The median split for D2.5 cm(3) (14.02 Gy) was also a significant predictor of toxicity (RR 6; P=.01). A highly significant logistic regression model was generated on the basis of D2.5 cm(3). One hundred percent (n = 7) of grade ≥4 toxicities were associated with radiation recall reactions after doxorubicin or gemcitabine chemotherapy or iatrogenic manipulation of the irradiated esophagus.
Conclusions: High-dose, single-fraction paraspinal SRS has a low rate of grade ≥3 esophageal toxicity. Severe esophageal toxicity is minimized with careful attention to esophageal doses during treatment planning. Iatrogenic manipulation of the irradiated esophagus and systemic agents classically associated with radiation recall reactions are associated with development of grade ≥4 toxicity.
Copyright © 2012 Elsevier Inc. All rights reserved.
Conflict of interest statement
Drs. Cox and Bilsky have no actual or potential conflicts of interest.
Figures


References
-
- Ryu SI, Chang SD, Kim DH, et al. Image-guided hypo-fractionated stereotactic radiosurgery to spinal lesions. Neurosurgery. 2001;49:838–846. - PubMed
-
- Yamada Y, Bilsky MH, Lovelock DM, et al. High-dose, single-fraction image-guided intensity-modulated radiotherapy for metastatic spinal lesions. Int J Radiat Oncol Biol Phys. 2008;71:484–490. - PubMed
-
- Gerszten PC, Burton SA, Ozhasoglu C, et al. Radiosurgery for spinal metastases: clinical experience in 500 cases from a single institution. Spine (Phila Pa 1976) 2007;32:193–199. - PubMed
-
- Gibbs IC, Kamnerdsupaphon P, Ryu MR, et al. Image-guided robotic radiosurgery for spinal metastases. Radiother Oncol. 2007;82:185–190. - PubMed
-
- Katagiri H, Takahashi M, Inagaki J, et al. Clinical results of nonsurgical treatment for spinal metastases. Int J Radiat Oncol Biol Phys. 1998;42:1127–1132. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
