

Multisite randomized trial of a single-session versus multisession literacy-sensitive self-care intervention for patients with heart failure
- PMID: 22572916
- PMCID: PMC3400336
- DOI: 10.1161/CIRCULATIONAHA.111.081745
Multisite randomized trial of a single-session versus multisession literacy-sensitive self-care intervention for patients with heart failure
Abstract
Background: Self-care training can reduce hospitalization for heart failure (HF), and more intensive intervention may benefit more vulnerable patients, including those with low literacy.
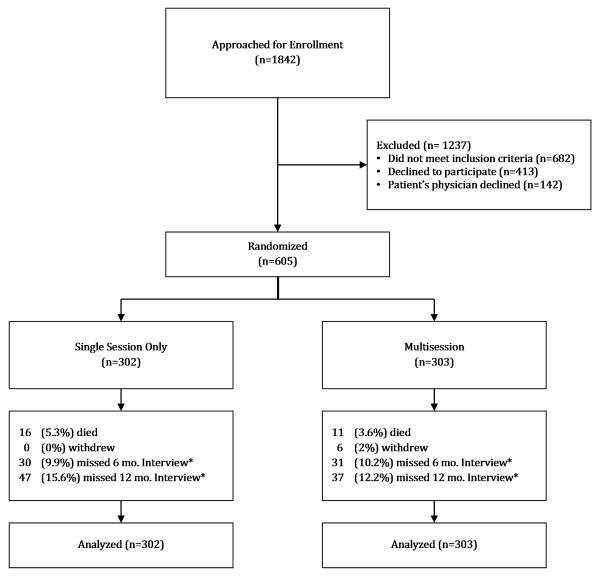
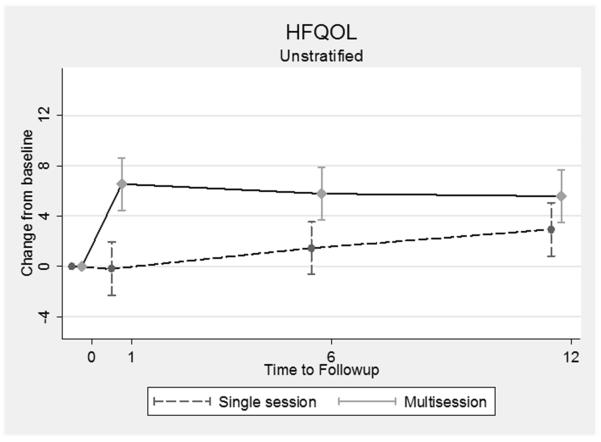
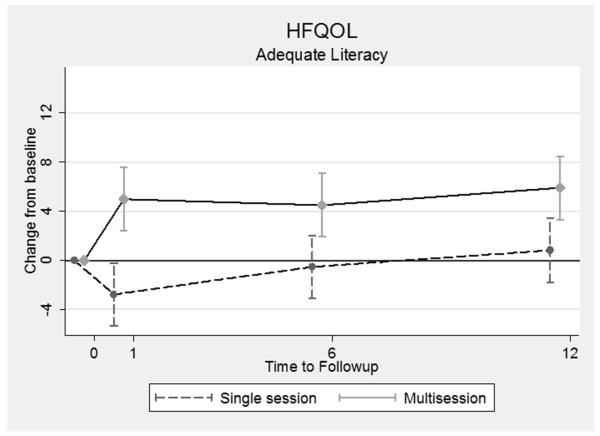
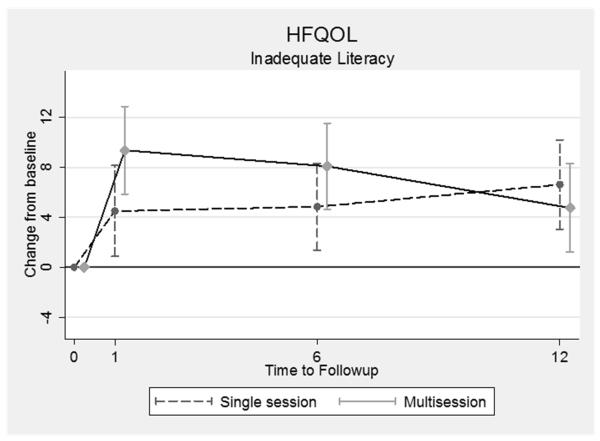
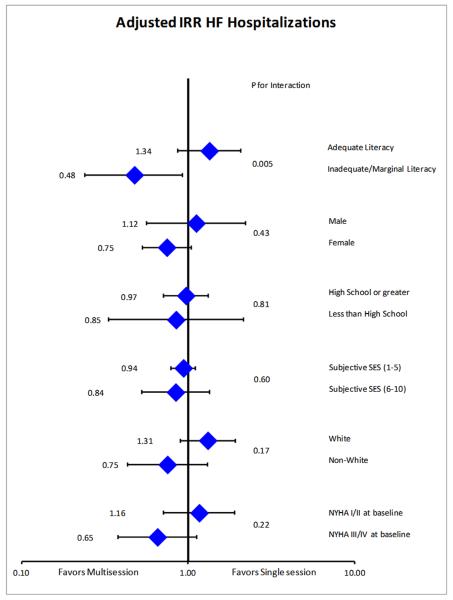
Methods and results: A 1-year, multisite, randomized, controlled comparative effectiveness trial with 605 patients with HF was conducted. Those randomized to a single session received a 40-minute in-person, literacy-sensitive training; the multisession group received the same initial training and then ongoing telephone-based support. The primary outcome was combined incidence of all-cause hospitalization or death; secondary outcomes included HF-related hospitalization and HF-related quality of life, with prespecified stratification by literacy. Overall, the incidence of all-cause hospitalization and death did not differ between intervention groups (incidence rate ratio, 1.01; 95% confidence interval, 0.83-1.22). The effect of multisession training compared with single-session training differed by literacy group: Among those with low literacy, the multisession training yielded a lower incidence of all-cause hospitalization and death (incidence rate ratio, 0.75; 95% confidence interval, 0.45-1.25), and among those with higher literacy, the multisession intervention yielded a higher incidence (incidence rate ratio, 1.22; 95% confidence interval, 0.99-1.50; interaction P=0.048). For HF-related hospitalization, among those with low literacy, multisession training yielded a lower incidence (incidence rate ratio, 0.53; 95% confidence interval, 0.25-1.12), and among those with higher literacy, it yielded a higher incidence (incidence rate ratio, 1.32; 95% confidence interval, 0.92-1.88; interaction P=0.005). HF-related quality of life improved more for patients receiving multisession than for those receiving single-session interventions at 1 and 6 months, but the difference at 12 months was smaller. Effects on HF-related quality of life did not differ by literacy.
Conclusions: Overall, an intensive multisession intervention did not change clinical outcomes compared with a single-session intervention. People with low literacy appear to benefit more from multisession interventions than people with higher literacy.
Clinical trial registration: URL: http://www.clinicaltrials.gov. Unique identifier: NCT00378950.
Figures
References
-
- McAlister FA, Stewart S, Ferrua S, McMurray JJ. Multidisciplinary strategies for the management of heart failure patients at high risk for admission a systematic review of randomized trials. J Am Coll Cardiol. 2004;44:810–819. - PubMed
-
- Inglis SC, Clark RA, McAlister FA, Ball J, Lewinter C, Cullington D, Stewart S, Cleland JG. Structured telephone support or telemonitoring programmes for patients with chronic heart failure. Cochrane Database Syst Rev. 2010 CD007228. - PubMed
-
- Chan DC, Heidenreich PA, Weinstein MC, Fonarow GC. Heart failure disease management programs: A cost-effectiveness analysis. Am Heart J. 2008;155:332–338. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
