

Performance of 3-dimensional echocardiography in measuring left ventricular volumes and ejection fraction: a systematic review and meta-analysis
- PMID: 22575319
- PMCID: PMC3773600
- DOI: 10.1016/j.jacc.2012.01.037
Performance of 3-dimensional echocardiography in measuring left ventricular volumes and ejection fraction: a systematic review and meta-analysis
Abstract
Objectives: The primary aim of this systematic review is to objectively evaluate the test performance characteristics of three-dimensional echocardiography (3DE) in measuring left ventricular (LV) volumes and ejection fraction (EF).
Background: Despite its growing use in clinical laboratories, the accuracy of 3DE has not been studied on a large scale. It is unclear if this technology offers an advantage over traditional two-dimensional (2D) methods.
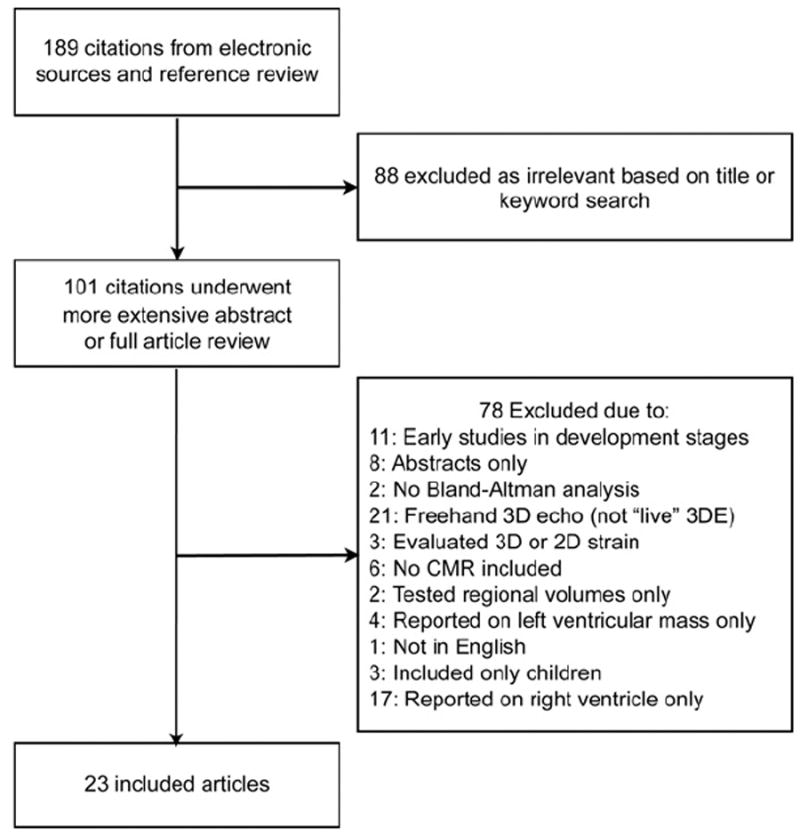
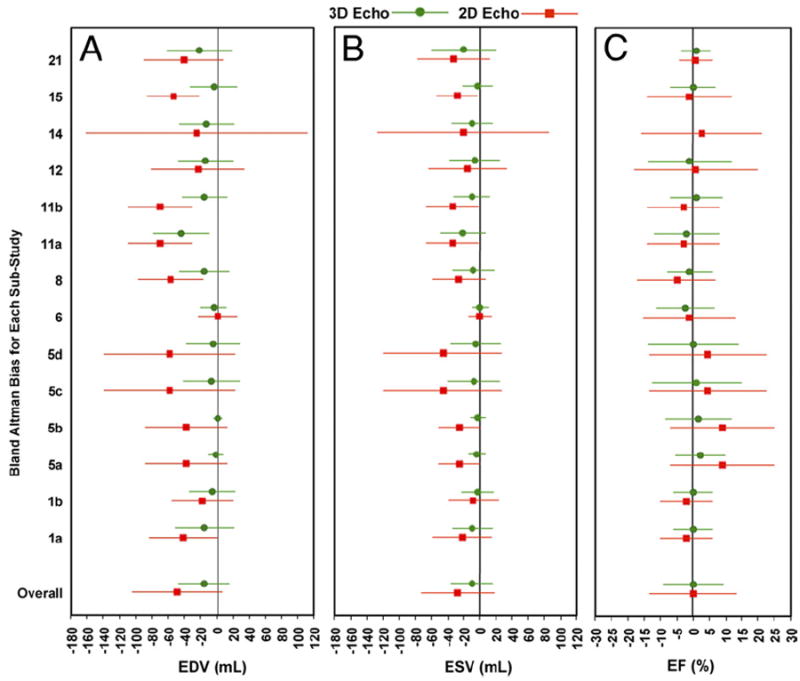
Methods: We searched for studies that compared LV volumes and EF measured by 3DE and cardiac magnetic resonance (CMR) imaging. A subset of those also compared standard 2D methods with CMR. We used meta-analyses to determine the overall bias and limits of agreement of LV end-diastolic volume (EDV), end-systolic volume (ESV), and EF measured by 3DE and 2D echocardiography (2DE).
Results: Twenty-three studies (1,638 echocardiograms) were included. The pooled biases ± 2 SDs for 3DE were -19.1 ± 34.2 ml, -10.1 ± 29.7 ml, and - 0.6 ± 11.8% for EDV, ESV, and EF, respectively. Nine studies also included data from 2DE, where the pooled biases were -48.2 ± 55.9 ml, -27.7 ± 45.7 ml, and 0.1 ± 13.9% for EDV, ESV, and EF, respectively. In this subset, the difference in bias between 3DE and 2D volumes was statistically significant (p = 0.01 for both EDV and ESV). The difference in variance was statistically significant (p < 0.001) for all 3 measurements.
Conclusions: Three-dimensional echocardiography underestimates volumes and has wide limits of agreement, but compared with traditional 2D methods in these carefully performed studies, 3DE is more accurate for volumes and more precise in all 3 measurements.
Copyright © 2012 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures



References
-
- Bonow RO, Carabello BA, Chatterjee K, et al. 2008 focused update incorporated into the ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 1998 Guidelines for the Management of Patients With Valvular Heart Disease). Endorsed by the Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. J Am Coll Cardiol. 2008;52:e1–142. - PubMed
-
- Moss AJ, Zareba W, Hall WJ, et al. Prophylactic implantation of a defibrillator in patients with myocardial infarction and reduced ejection fraction. N Engl J Med. 2002;346:877–83. - PubMed
-
- Packer M, Fowler MB, Roecker EB, et al. Effect of carvedilol on the morbidity of patients with severe chronic heart failure: results of the carvedilol prospective randomized cumulative survival (COPERNICUS) study. Circulation. 2002;106:2194–9. - PubMed
-
- Young JB, Abraham WT, Smith AL, et al. Combined cardiac resynchronization and implantable cardioversion defibrillation in advanced chronic heart failure: the MIRACLE ICD Trial. JAMA. 2003;289:2685–94. - PubMed
-
- SOLVD Investigators. Effect of enalapril on mortality and the development of heart failure in asymptomatic patients with reduced left ventricular ejection fractions. N Engl J Med. 1992;327:685–91. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
