

E-prostanoid 2 receptor signaling suppresses lung innate immunity against Streptococcus pneumoniae
- PMID: 22575745
- PMCID: PMC3350638
- DOI: 10.1016/j.prostaglandins.2012.03.002
E-prostanoid 2 receptor signaling suppresses lung innate immunity against Streptococcus pneumoniae
Abstract
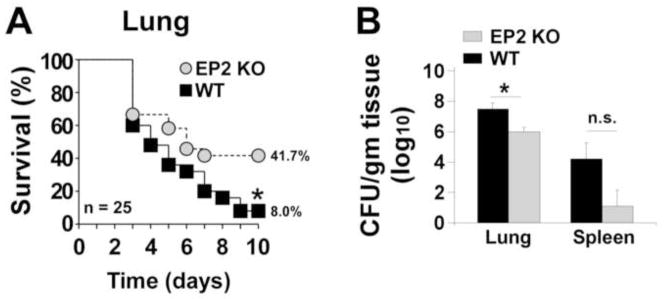
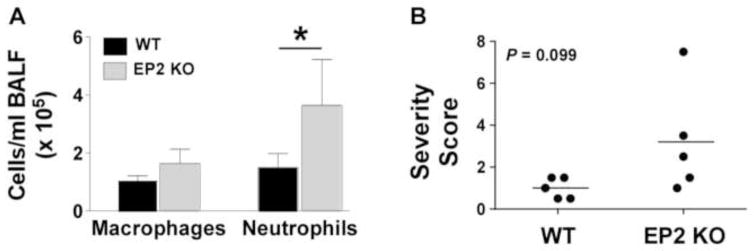
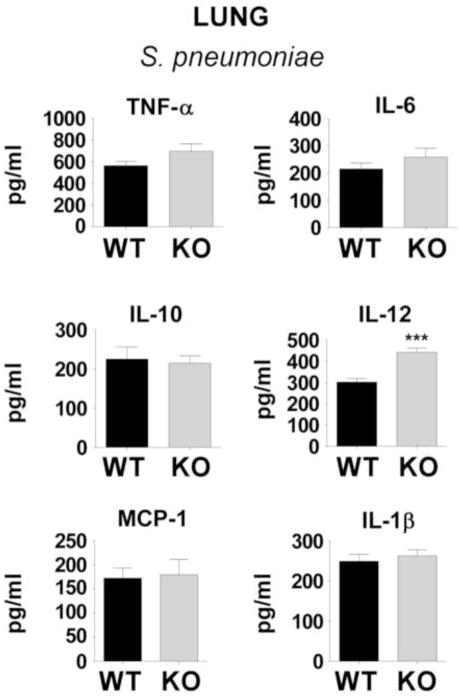
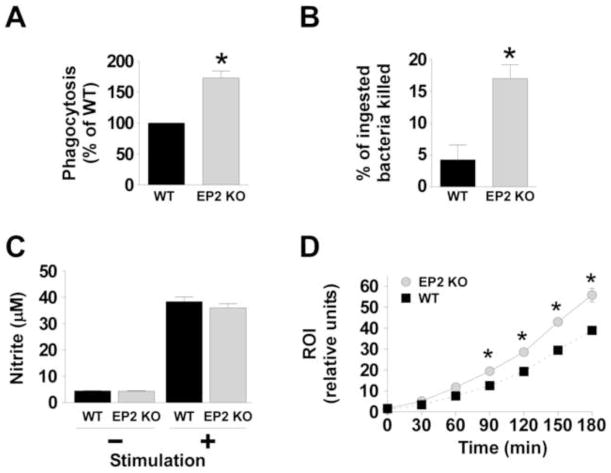
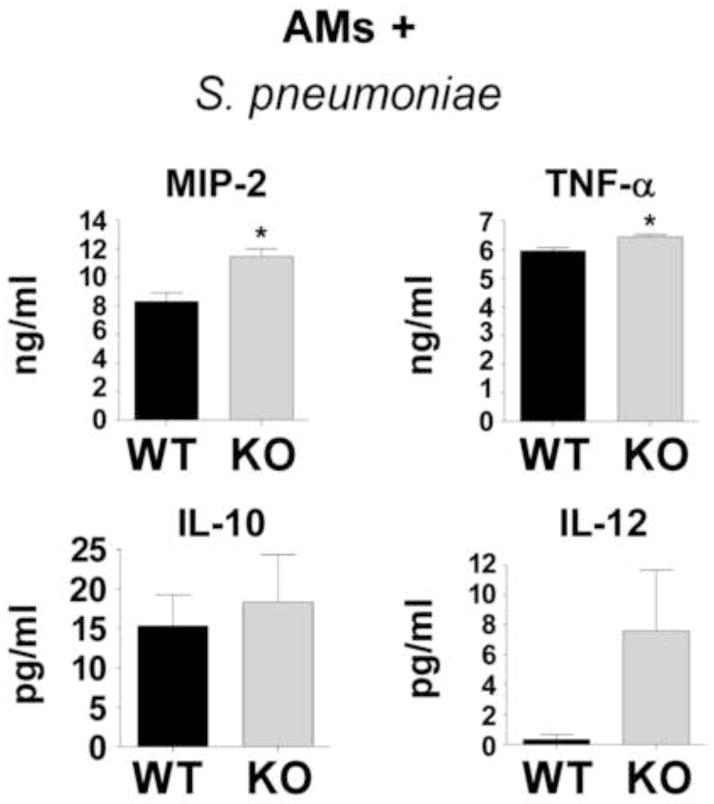
Pneumonia is a major global health problem. Prostaglandin (PG) E(2) is an immunomodulatory lipid with anti-inflammatory, immunosuppressive, and pro-resolving actions. Data suggest that the E-prostanoid (EP) 2 receptor mediates immunomodulatory effects of PGE(2), but the extent to which this occurs in Streptococcus pneumoniae infection is unknown. Intratracheal lung infection of C57BL/6 mice possessing (EP2(+/+)) or lacking (EP2(-/-)) the EP2 receptor was performed, as were in vitro studies of alveolar macrophage (AM) host defense functions. Bacterial clearance and survival were significantly improved in vivo in EP2(-/-) mice and it correlated with greater neutrophilic inflammation and higher lung IL-12 levels. Upon ex vivo challenge with pneumococcus, EP2(-/-)cells expressed greater amounts of TNF-α and MIP-2 than did EP2(+/+) AMs, and had improved phagocytosis, intracellular killing, and reactive oxygen intermediate generation. These data suggest that PGE(2)-EP2 signaling may provide a novel pharmacological target for treating pneumococcal pneumonia in combination with antimicrobials.
Copyright © 2012 Elsevier Inc. All rights reserved.
Conflict of interest statement
All the authors declare that they have no competing interests.
Figures
References
-
- Bernstein A, Bilheimer LT, Makuc DM. National Center for Health, S. Dept. of Health and Human Services, Centers for Disease Control and Prevention, National Center for Health Statistics. Hyattsville, MD: 2011.
-
- Bosso JA, Drew RH. Application of antimicrobial stewardship to optimise management of community acquired pneumonia. Int J Clin Pract. 2011;65(7):775–83. - PubMed
-
- Levine OS, O’Brien KL, Knoll M, et al. Pneumococcal vaccination in developing countries. Lancet. 2006;367(9526):1880–2. - PubMed
-
- Kadioglu A, Andrew PW. The innate immune response to pneumococcal lung infection: the untold story. Trends Immunol. 2004;25(3):143–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
