

Resection of hepatocellular cancer ≤2 cm: results from two Western centers
- PMID: 22576353
- PMCID: PMC3442120
- DOI: 10.1002/hep.25832
Resection of hepatocellular cancer ≤2 cm: results from two Western centers
Abstract
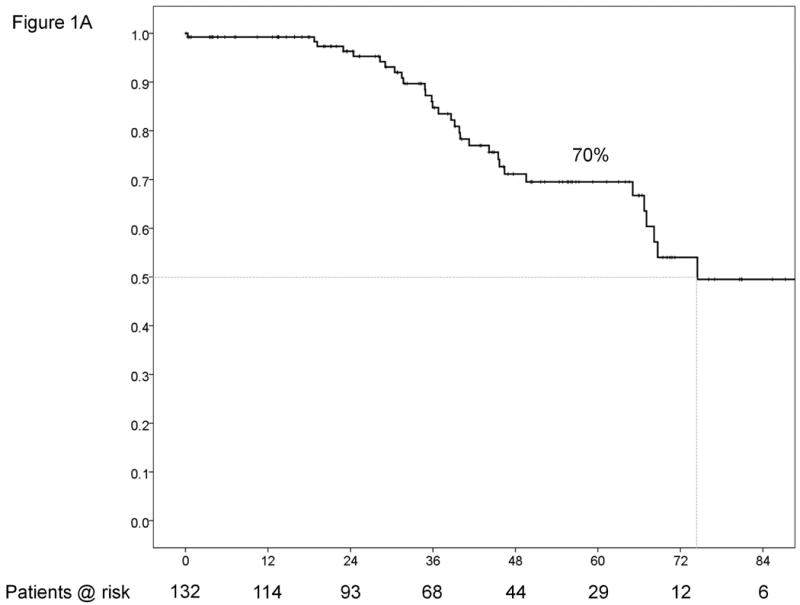
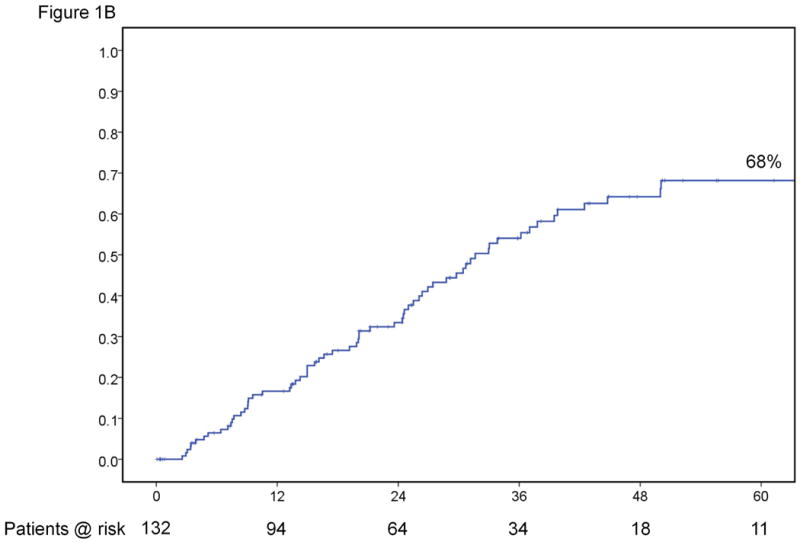
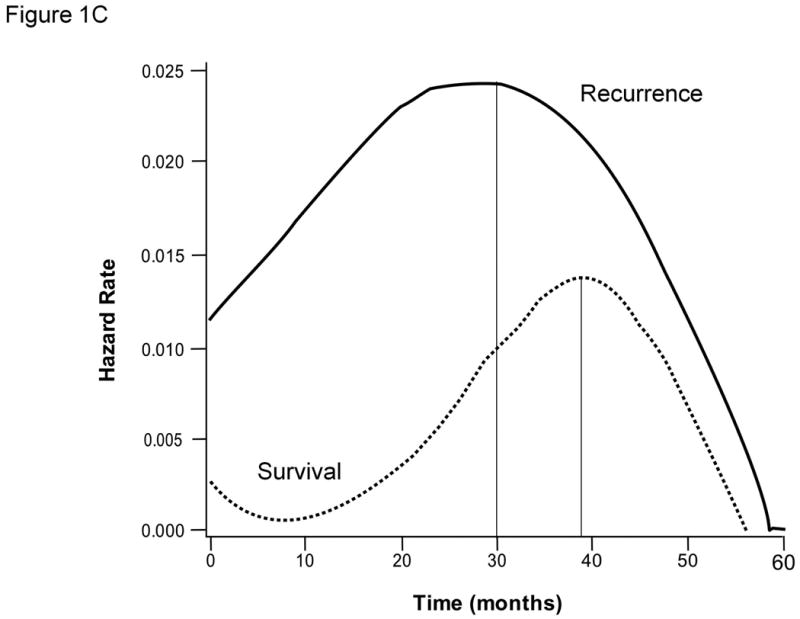
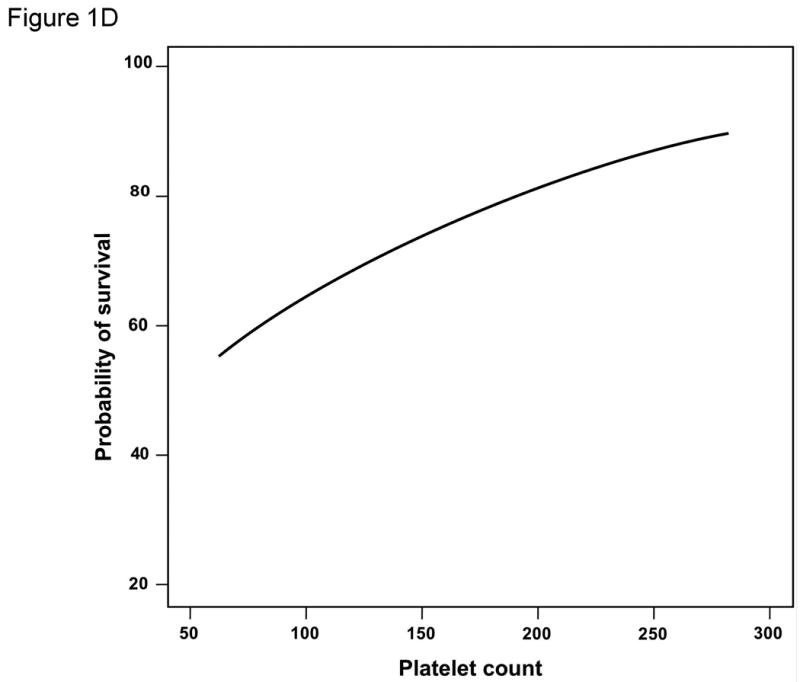
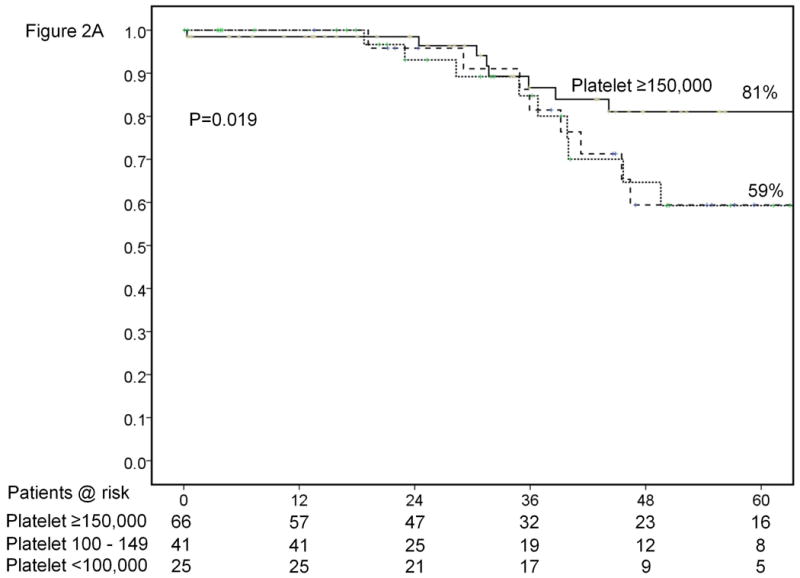
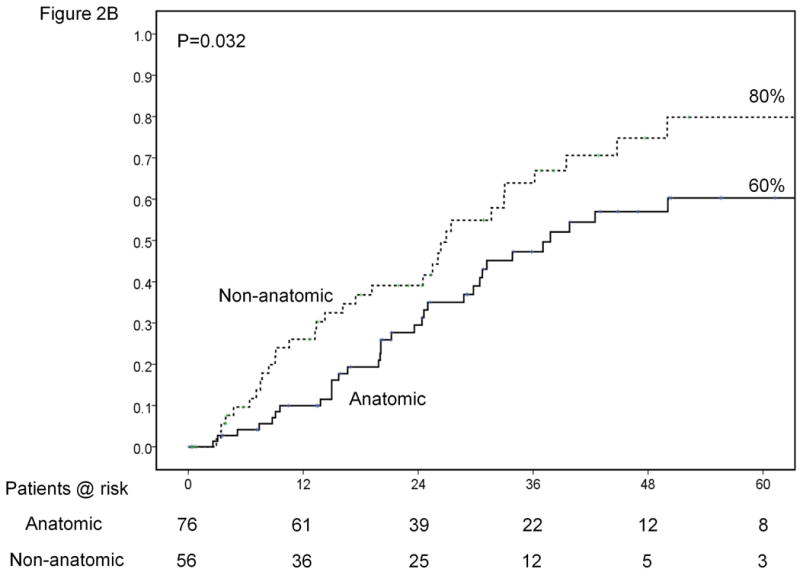
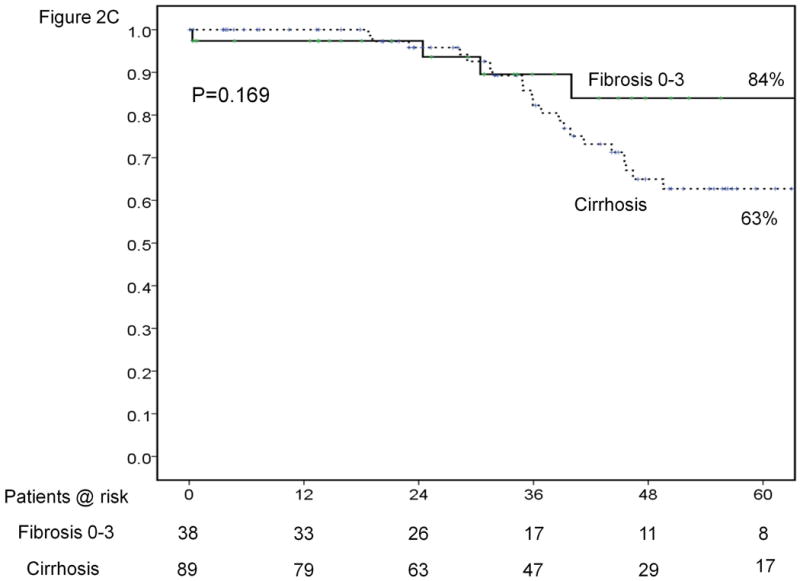
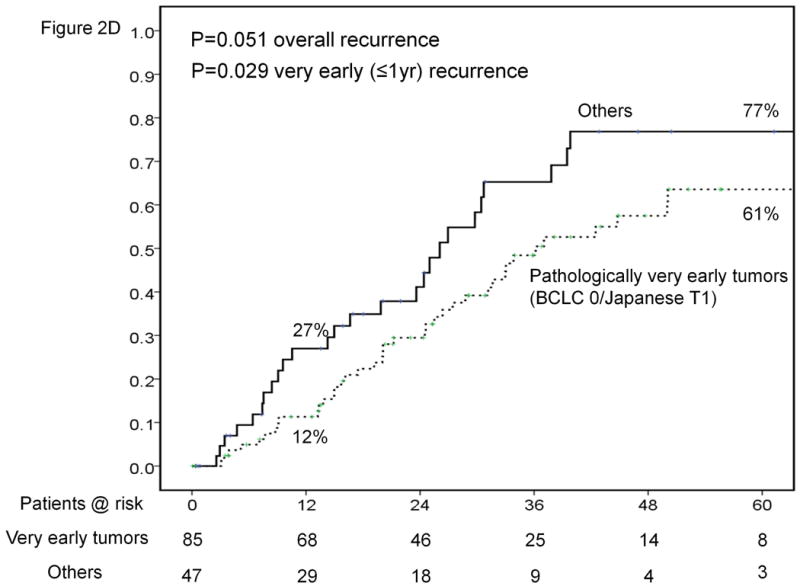
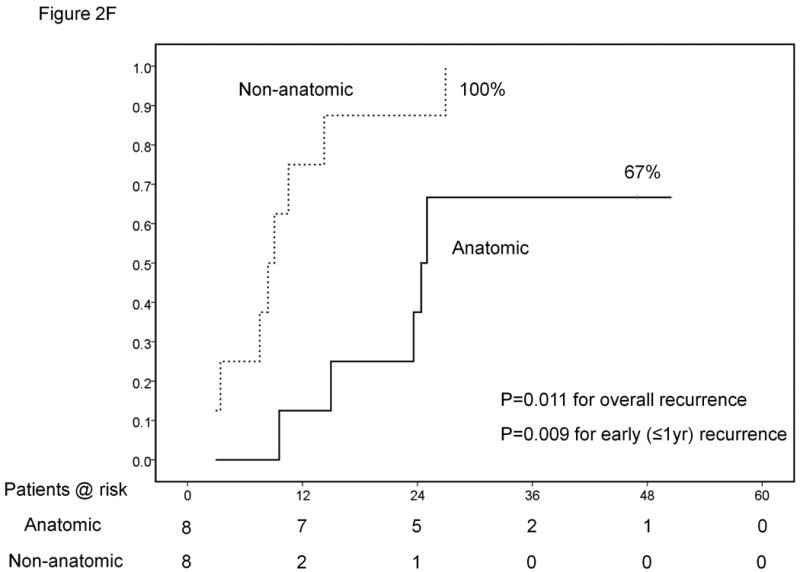
Asian series have shown a 5-year survival rate of ≈70% after resection of hepatocellular carcinoma (HCC) ≤2 cm. Western outcomes with resection have not been as good. In addition, ablation of HCC ≤2 cm has been shown to achieve competitive results, leaving the role of resection in these patients unclear. Records of patients undergoing resection at two Western centers between January 1990 and December 2009 were reviewed. Patients with a single HCC ≤2 cm on pathologic analysis were included. Thirty clinical variables including demographics, liver function, tumor characteristics, nature of the surgery, and the surrounding liver were examined. An exploratory statistical analysis was conducted to determine variables associated with recurrence and survival. The study included 132 patients with a median follow-up of 37.5 months. There was one (<1%) 90-day mortality. There were 32 deaths with a median survival of 74.5 months and a 5-year survival rate of 70% (63% in patients with cirrhosis). The median time to recurrence was 31.6 months and the 5-year recurrence rate was 68%. Presence of satellites (hazard ratio [HR], 2.46; P = 0.031) and platelet count <150,000/μL (HR, 2.37; P = 0.026) were independently associated with survival. Presence of satellites (HR, 2.79; P = 0.003), cirrhosis (HR, 2.3; P = 0.010), and nonanatomic resection (HR, 1.79; P = 0.031) were independently associated with recurrence. Patients with a single HCC ≤2 cm and platelet count ≥150,000/μL achieved a median survival of 138 months and a 5-year survival rate of 8%, respectively.
Conclusion: Resection of HCC ≤2 cm is safe and achieves excellent results in Western centers. Recurrence continues to be a significant problem. Presence of satellites, platelet count, anatomic resection, and cirrhosis are associated with outcomes after resection, even among such early tumors. Resection should continue to be considered a primary treatment modality in patients with small HCC and well-preserved liver function.
Copyright © 2013 American Association for the Study of Liver Diseases.
Figures

Comment in
-
Toward a rational management of very early hepatocellular carcinoma.Hepatology. 2013 Apr;57(4):1300-2. doi: 10.1002/hep.26074. Epub 2013 Mar 6. Hepatology. 2013. PMID: 22987787 No abstract available.
-
Reply:Hepatology. 2013 Jul;58(1):452-3. doi: 10.1002/hep.26241. Epub 2013 May 28. Hepatology. 2013. PMID: 23315707 No abstract available.
-
The role of biopsy of the nontumorous liver parenchyma in patients considered for partial resection of small hepatocellular carcinoma.Hepatology. 2013 Jul;58(1):452. doi: 10.1002/hep.26244. Epub 2013 May 27. Hepatology. 2013. PMID: 23315837 No abstract available.
-
Platelet count and survival of patients with compensated cirrhosis and small hepatocellular carcinoma treated with surgery.Hepatology. 2014 Apr;59(4):1649. doi: 10.1002/hep.26622. Epub 2014 Feb 18. Hepatology. 2014. PMID: 23857512 No abstract available.
-
Reply: To PMID 22576353.Hepatology. 2014 Apr;59(4):1653-4. doi: 10.1002/hep.26688. Epub 2014 Feb 18. Hepatology. 2014. PMID: 23959942 No abstract available.
-
A comparison of surgical resection and radiofrequency ablation for the treatment of single small hepatocellular carcinoma ≤2 cm.Hepatology. 2014 Apr;59(4):1653. doi: 10.1002/hep.26692. Epub 2014 Feb 18. Hepatology. 2014. PMID: 24038056 No abstract available.
References
-
- Llovet JM, Burroughs A, Bruix J. Hepatocellular carcinoma. Lancet. 2003;362(9399):1907–1917. - PubMed
-
- Liver Cancer Study Group of Japan. General Rules for the Clinical and Pathological Study of Primary Liver Cancer. Kanehara. 2003 - PubMed
-
- Bruix J, Sherman M, Llovet JM, Beaugrand M, Lencioni R, Burroughs AK, Christensen E, et al. Clinical management of hepatocellular carcinoma. conclusions of the barcelona-2000 EASL conference. european association for the study of the liver. J Hepatol. 2001;35(3):421–430. - PubMed
-
- Bruix J, Sherman M. Practice Guidelines Committee, American Association for the Study of Liver Diseases. Management of hepatocellular carcinoma. Hepatology. 2005;42(5):1208–1236. - PubMed
-
- Forner A, Vilana R, Ayuso C, Bianchi L, Sole M, Ayuso JR, Boix L, et al. Diagnosis of hepatic nodules 20 mm or smaller in cirrhosis: Prospective validation of the noninvasive diagnostic criteria for hepatocellular carcinoma. Hepatology. 2008;47(1):97–104. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical