

Hospital percutaneous coronary intervention appropriateness and in-hospital procedural outcomes: insights from the NCDR
- PMID: 22576845
- PMCID: PMC3520092
- DOI: 10.1161/CIRCOUTCOMES.112.966044
Hospital percutaneous coronary intervention appropriateness and in-hospital procedural outcomes: insights from the NCDR
Abstract
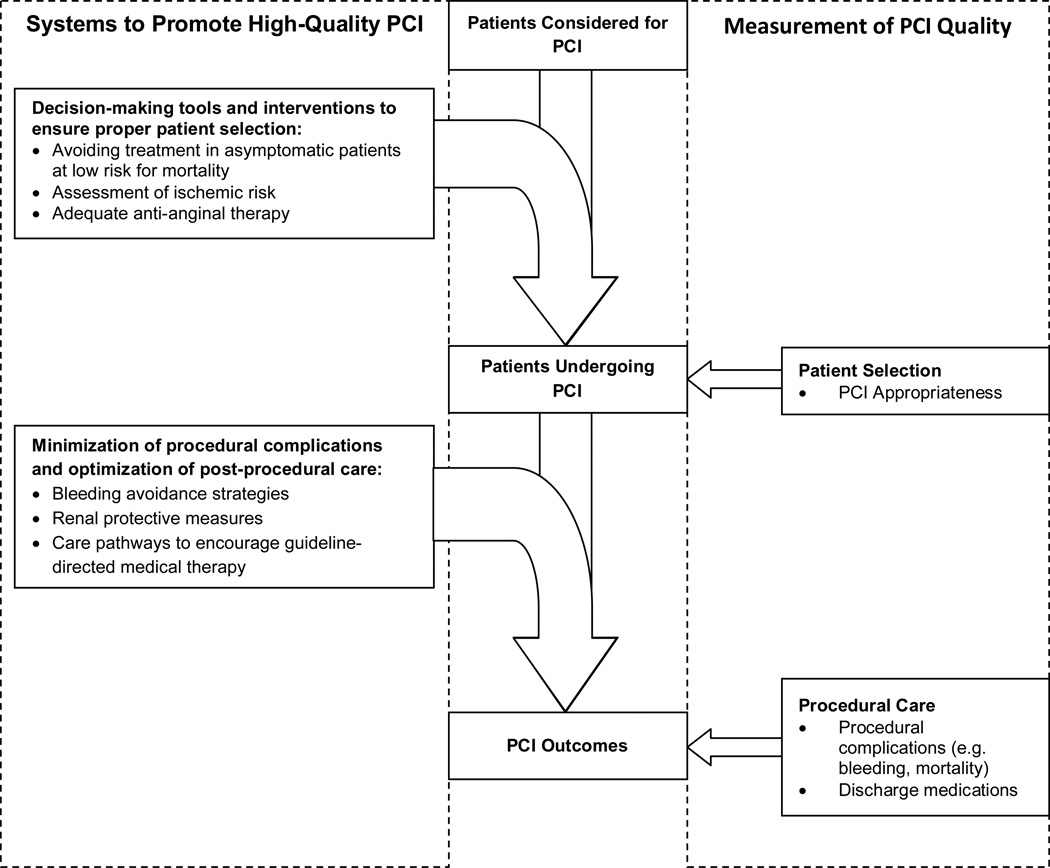
Background: Measurement of hospital quality has traditionally focused on processes of care and postprocedure outcomes. Appropriateness measures for percutaneous coronary intervention (PCI) assess quality as it relates to patient selection and the decision to perform PCI. The association between patient selection for PCI and processes of care and postprocedural outcomes is unknown.
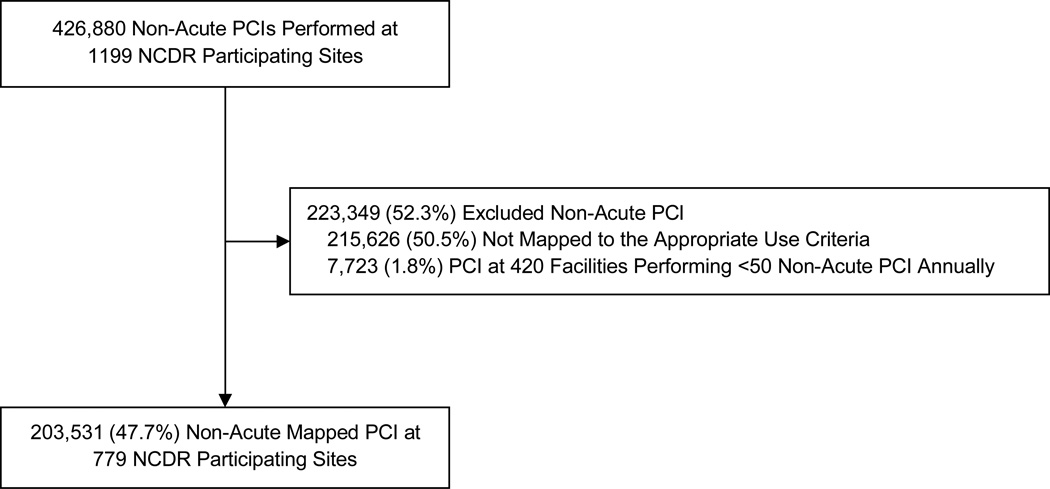
Methods and results: We included 203 531 patients undergoing nonacute (elective) PCI from 779 hospitals participating in the National Cardiovascular Data Registry (NCDR) CathPCI Registry between July 2009 and April 2011. We examined the association between a hospital's proportion of nonacute PCIs categorized as inappropriate by the 2009 Appropriate Use Criteria (AUC) for Coronary Revascularization and in-hospital mortality, bleeding complications, and use of optimal guideline-directed medical therapy at discharge (ie, aspirin, thienopyridines, and statins). When categorized as hospital tertiles, the range of inappropriate PCI was 0.0% to 8.1% in the lowest tertile, 8.1% to 15.2% in the middle tertile, and 15.2% to 58.6% in the highest tertile. Compared with lowest-tertile hospitals, mortality was not significantly different at middle-tertile (adjusted odds ratio [OR], 0.93; 95% confidence interval [CI], 0.73-1.19) or highest-tertile hospitals (OR, 1.12; 95% CI, 0.88-1.43; P=0.35 for differences between tertiles). Similarly, risk-adjusted bleeding did not vary significantly (middle-tertile OR, 1.13; 95% CI, 1.02-1.16; highest-tertile OR, 1.02; 95% CI, 0.91-1.16; P=0.07 for differences between tertiles) nor did use of optimal medical therapy at discharge (85.3% versus 85.7% versus 85.2%; P=0.58).
Conclusions: In a national cohort of nonacute PCIs, a hospital's proportion of inappropriate PCIs was not associated with in-hospital mortality, bleeding, or medical therapy at discharge. This suggests PCI appropriateness measures aspects of hospital PCI quality that are independent of how well the procedure is performed. Therefore, PCI appropriateness and postprocedural outcomes are both important metrics to inform PCI quality.
Conflict of interest statement
Dr. Bradley had full access to all of the data in the study and takes full responsibility for the integrity of the data and the accuracy of the data analysis.
Conflict of Interest Disclosures: The authors report no relevant disclosures.
Role of the Sponsor: Because the ACC oversees the NCDR, it funded the collection of data in the CathPCI registry, and representatives of the CathPCI Research and Publications committee approved the final manuscript.
Disclaimers: The views expressed in this manuscript represent those of the authors, and do not necessarily represent the official views of the NCDR or its associated professional societies identified at
Figures
References
-
- Frey P, Connors A, Resnic FS. Quality measurement and improvement in the cardiac catheterization laboratory. Circulation. 2012;125:615–619. - PubMed
-
- Bradley EH, Nallamothu BK, Herrin J, Ting HH, Stern AF, Nembhard IM, Yuan CT, Green JC, Kline-Rogers E, Wang Y, Curtis JP, Webster TR, Masoudi FA, Fonarow GC, Brush JE, Jr, Krumholz HM. National efforts to improve door-to-balloon time results from the Door-to-Balloon Alliance. J Am Coll Cardiol. 2009;54:2423–2429. - PubMed
-
- Dehmer GJ, Elma M, Hewitt K, Brindis RG. Bringing measurement and management science to the cath laboratory: the National Cardiovascular Data Registry (ACC-NCDR) and the Cardiac Catheterization Laboratory Continuous Quality Improvement Toolkit (ACC-CathKIT) J Cardiovasc Manag. 2004;15:20–26. - PubMed
-
- Patel MR, Dehmer GJ, Hirshfeld JW, Smith PK, Spertus JA. ACCF/SCAI/STS/AATS/AHA/ASNC 2009 Appropriateness Criteria for Coronary Revascularization: a report by the American College of Cardiology Foundation Appropriateness Criteria Task Force, Society for Cardiovascular Angiography and Interventions, Society of Thoracic Surgeons, American Association for Thoracic Surgery, American Heart Association, and the American Society of Nuclear Cardiology Endorsed by the American Society of Echocardiography, the Heart Failure Society of America, and the Society of Cardiovascular Computed Tomography. J Am Coll Cardiol. 2009;53:530–553. - PubMed
-
- NCDR® CathPCI Registry®. [Accessed: January 12, 2012]; Available at: https://www.ncdr.com/webncdr/DefaultCathPCI.aspx.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
