

Effects of circuit training as alternative to usual physiotherapy after stroke: randomised controlled trial
- PMID: 22577186
- PMCID: PMC3349299
- DOI: 10.1136/bmj.e2672
Effects of circuit training as alternative to usual physiotherapy after stroke: randomised controlled trial
Abstract
Objective: To analyse the effect of task oriented circuit training compared with usual physiotherapy in terms of self reported walking competency for patients with stroke discharged from a rehabilitation centre to their own home.
Design: Randomised controlled trial with follow-up to 24 weeks.
Setting: Multicentre trial in nine outpatient rehabilitation centres in the Netherlands
Participants: Patients with stroke who were able to walk a minimum of 10 m without physical assistance and were discharged from inpatient rehabilitation to an outpatient rehabilitation clinic. Patients were randomly allocated to circuit training or usual physiotherapy, after stratification by rehabilitation centre, with an online randomisation procedure.
Intervention: Patients in the intervention group received circuit training in 90 minute sessions twice a week for 12 weeks. The training included eight different workstations in a gym and was intended to improve performance in tasks relating to walking competency. The control group received usual outpatient physiotherapy.
Main outcome measures: The primary outcome was the mobility domain of the stroke impact scale (SIS, version 3.0). Secondary outcomes were standing balance, self reported abilities, gait speed, walking distance, stair climbing, instrumental activities of daily living, fatigue, anxiety, and depression. Differences between groups were analysed according to the intention to treat principle. All outcomes were assessed by blinded observers in a repeated measurement design lasting 24 weeks.
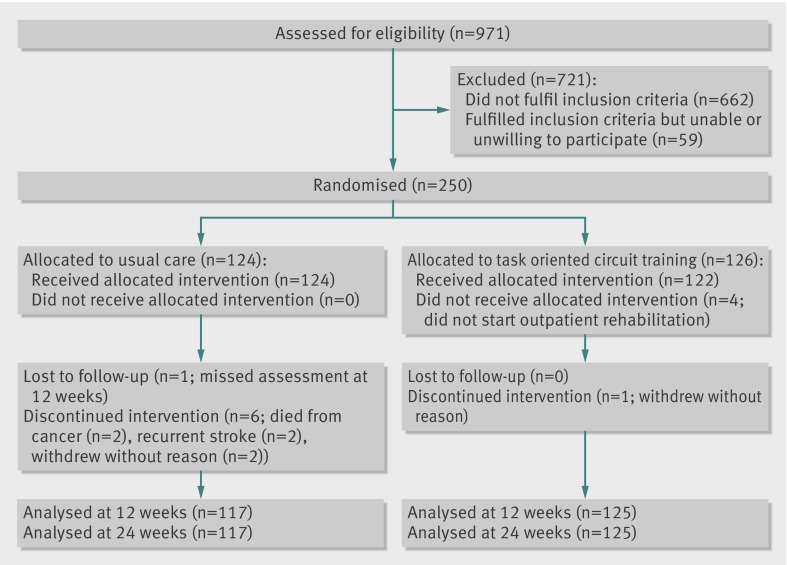
Results: 126 patients were included in the circuit training group and 124 in the usual care group (control), with data from 125 and 117, respectively, available for analysis. One patient from the circuit training group and seven from the control group dropped out. Circuit training was a safe intervention, and no serious adverse events were reported. There were no significant differences between groups for the stroke impact scale mobility domain (β=0.05 (SE 0.68), P=0.943) at 12 weeks. Circuit training was associated with significantly higher scores in terms of gait speed (0.09 m/s (SE 0.02), P<0.001), walking distance (20.0 m (SE 7.4), P=0.007), and modified stairs test (-1.6 s (SE 0.7), P=0.015). There were no significant differences between groups for the other secondary outcomes, except for the leisure domain of the Nottingham extended activities of daily living and the memory and thinking domain of the stroke impact scale. With the exception of gait speed (-0.04 m/s (SE 0.02), P=0.040), there were no significant differences between groups at follow-up.
Conclusion: Task oriented circuit training can safely replace usual physiotherapy for patients with stroke who are discharged from inpatient rehabilitation to the community and need further training in gait and gait related activities as an outpatient.
Trial registration: Dutch Trial Register (NTR1534).
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures
Comment in
-
Group task-specific circuit training for patients discharged home after stroke may be as effective as individualised physiotherapy in improving mobility.J Physiother. 2012;58(4):269. doi: 10.1016/S1836-9553(12)70129-7. J Physiother. 2012. PMID: 23177230
References
-
- Lloyd-Jones D, Adams RJ, Brown TM, Carnethon M, Dai S, de Simone G, et al. Heart disease and stroke statistics—2010 update: a report from the American Heart Association. Circulation 2010;121:948-54. - PubMed
-
- Veerbeek JM, Kwakkel G, van Wegen EE, Ket JC, Heymans MW. Early prediction of outcome of activities of daily living after stroke: a systematic review. Stroke 2011;42:1482-8. - PubMed
-
- McKevitt C, Fudge N, Redfern J, Sheldenkar A, Crichton S, Rudd AR, et al. Self-reported long-term needs after stroke. Stroke 2011;42:1398-403. - PubMed
-
- Langhorne P, Bernhardt J, Kwakkel G. Stroke rehabilitation. Lancet 2011;377:1693-702. - PubMed
-
- Kwakkel G, van Peppen R, Wagenaar RC, Wood DS, Richards C, Ashburn A, et al. Effects of augmented exercise therapy time after stroke: a meta-analysis. Stroke 2004;35:2529-39. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical