

Autoantibody with Cross-Reactivity between Insulin and Ductal Cells May Cause Diabetic Mastopathy: A Case Study
- PMID: 22577391
- PMCID: PMC3346992
- DOI: 10.1155/2012/569040
Autoantibody with Cross-Reactivity between Insulin and Ductal Cells May Cause Diabetic Mastopathy: A Case Study
Abstract
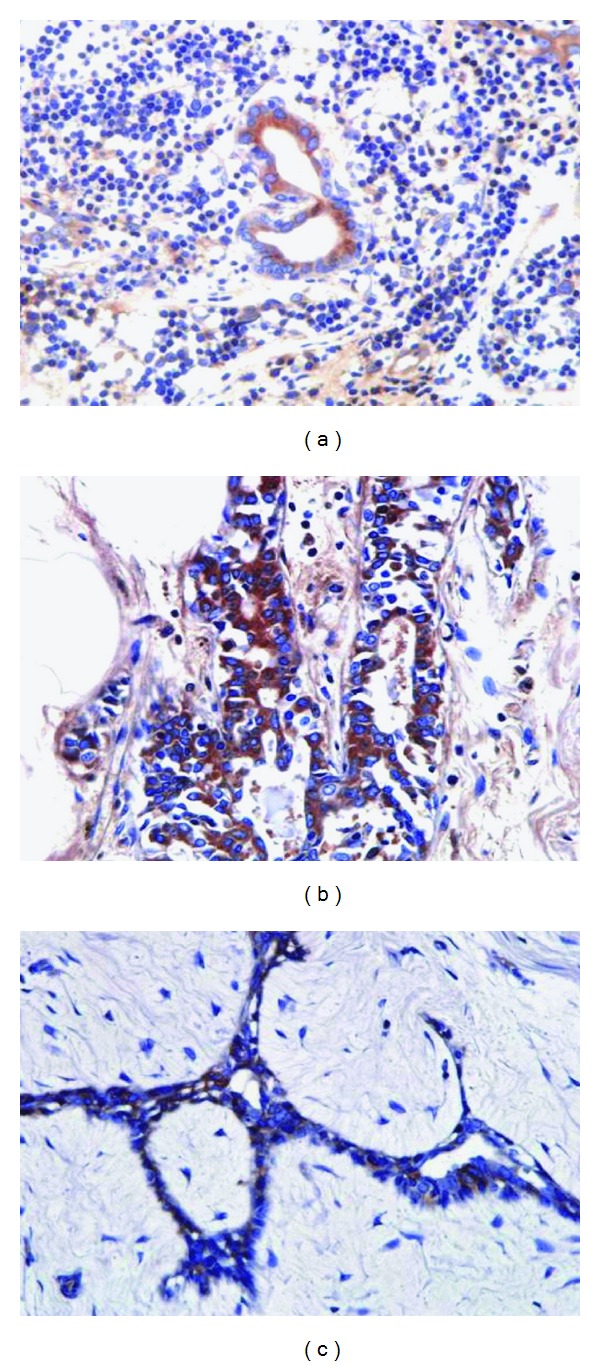
Lymphocytic mastopathy or diabetic mastopathy is a benign breast disease characterized by dense fibrosis, lobular atrophy, and aggregates of lymphocytes in a periductal and perilobular distribution. The condition usually affects women with a long history of diabetes mellitus (DM) and also those with autoimmune disorders. While the pathogenesis is unknown, a particular type of class II human leukocyte antigen has been associated with this disease. Herein, we report a case of diabetic mastopathy which clinically and radiologically mimicked primary breast neoplasms. The patient was a 74-year-old woman with a 31-year history of DM type II who presented with multiple firm lumps in bilateral breasts. Findings from mammography, ultrasonography, and magnetic resonance imaging of the breasts revealed an abnormal appearance which suspiciously resembled malignancy. An aspiration cytology specimen showed atypical accumulation of lymphoid cells, leading us to suspect lymphoma. Histology of an excisional biopsy showed the characteristic appearance of lymphocytic mastopathy, which predominantly consisted of B-lymphocytes. Autoantibodies in her serum reacted positively against her ductal epithelium as well as other diabetic and nondiabetic breast ductal cells. An antigen absorption test with insulin revealed attenuating intensity according to insulin concentration. These anti-insulin antibodies produced in the DM patient may cause ductitis because of antigen cross-reactivity.
Figures







References
-
- Soler N, Khardori R. Fibrous disease of the breast, thyroiditis, and cheiroarthropathy in type I diabetes mellitus. The Lancet. 1984;1(8370):193–195. - PubMed
-
- Fong D, Lann MA, Finlayson C, Page DL, Singh M. Diabetic (lymphocytic) mastopathy with exuberant lymphohistiocytic and granulomatous response: a case report with review of the literature. American Journal of Surgical Pathology. 2006;30(10):1330–1336. - PubMed
-
- Lammie GA, Bobrow LG, Staunton MD, Levison DA, Page G, Millis RR. Sclerosing lymphocytic lobulitis of the breast—evidence for an autoimmune pathogenesis. Histopathology. 1991;19(1):13–20. - PubMed
-
- Tsutsumi Y, Hara M. Application of parietal cell autoantibody to histopathological studies. Acta Pathologica Japonica. 1985;35(4):823–829. - PubMed
-
- Valdez R, Thorson J, Finn WG, Schnitzer B, Kleer CG. Lymphocytic mastitis and diabetic mastopathy: a molecular, immunophenotypic, and clinicopathologic evaluation of 11 cases. Modern Pathology. 2003;16(3):223–228. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
