

Natural history of pediatric intestinal failure: initial report from the Pediatric Intestinal Failure Consortium
- PMID: 22578586
- PMCID: PMC3419777
- DOI: 10.1016/j.jpeds.2012.03.062
Natural history of pediatric intestinal failure: initial report from the Pediatric Intestinal Failure Consortium
Abstract
Objective: To characterize the natural history of intestinal failure (IF) among 14 pediatric centers during the intestinal transplantation era.
Study design: The Pediatric Intestinal Failure Consortium performed a retrospective analysis of clinical and outcome data for a multicenter cohort of infants with IF. Entry criteria included infants <12 months receiving parenteral nutrition (PN) for >60 continuous days. Enteral autonomy was defined as discontinuation of PN for >3 consecutive months. Values are presented as median (25th, 75th percentiles) or as number (%).
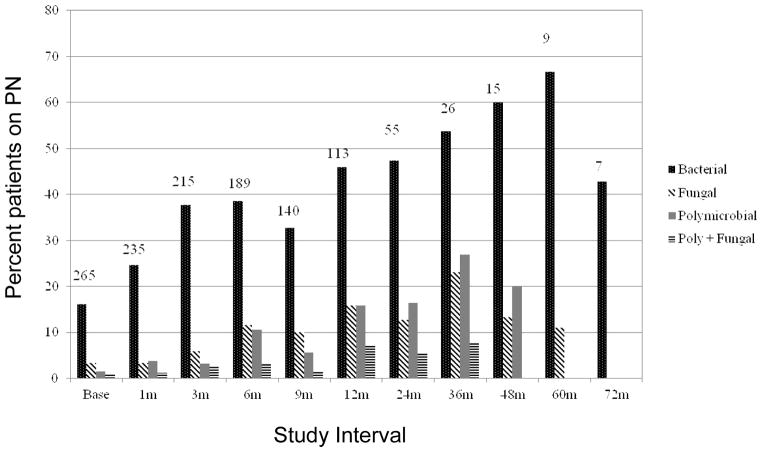
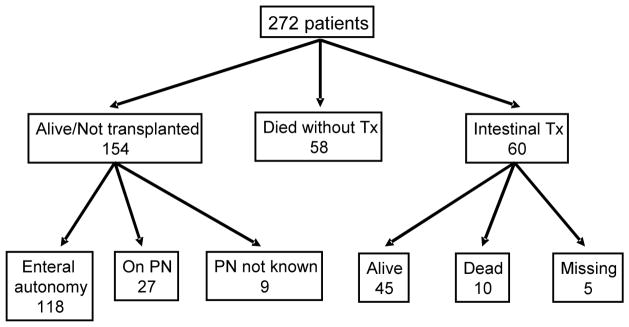
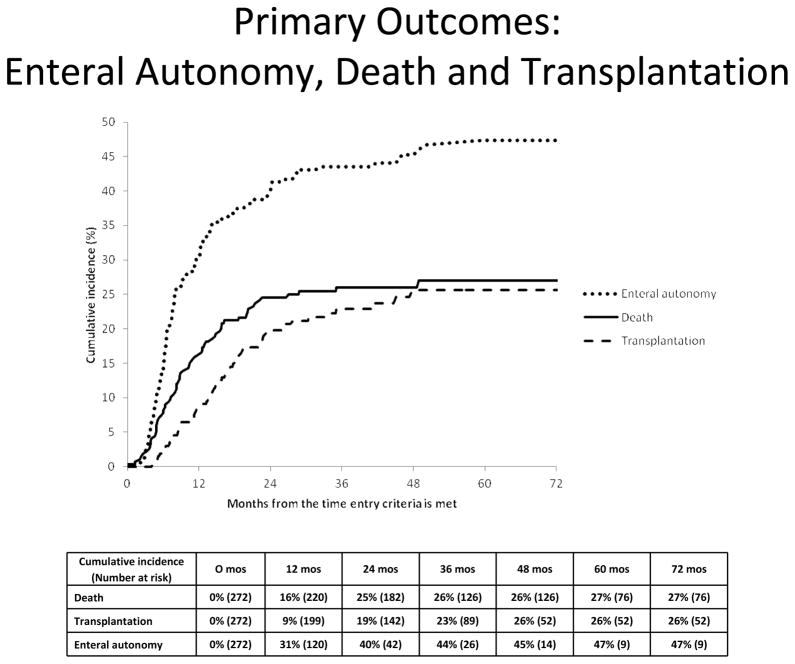
Results: 272 infants with a gestational age of 34 weeks (30, 36) and birth weight of 2.1 kg (1.2, 2.7) were followed for 25.7 months (11.2, 40.9). Residual small bowel length in 144 patients was 41 cm (25.0, 65.5). Diagnoses were necrotizing enterocolitis (71, 26%), gastroschisis (44, 16%), atresia (27, 10%), volvulus (24, 9%), combinations of these diagnoses (46, 17%), aganglionosis (11, 4%), and other single or multiple diagnoses (48, 18%). Prescribed medications included oral antibiotics (207, 76%), H2 blockers (187, 69%), and proton pump inhibitors (156, 57%). Enteral feeding approaches varied among centers; 19% of the cohort received human milk. The cohort experienced 8.9 new catheter-related blood stream infections per 1000 catheter days. The cumulative incidences for enteral autonomy, death, and intestinal transplantation were 47%, 27%, and 26%, respectively. Enteral autonomy continued into the fifth year after study entry.
Conclusions: Children with IF endure significant mortality and morbidity. Enteral autonomy may require years to achieve. Improved medical, nutritional, and surgical management may reduce time on PN, mortality, and need for transplantation.
Copyright © 2012 Mosby, Inc. All rights reserved.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Goulet O, Ruemmele F, Lacaille F, Colomb V. Irreversible intestinal failure. J Pediatr Gastroenterol Nutr. 2004 Mar;38:250–69. - PubMed
-
- Kocoshis SA, Beath SV, Booth IW, Garcia Oliva CA, Goulet O, Kaufman SS, et al. Intestinal failure and small bowel transplantation, including clinical nutrition: Working Group report of the second World Congress of Pediatric Gastroenterology, Hepatology, and Nutrition. J Pediatr Gastroenterol Nutr. 2004 Jun;39( Suppl 2):S655–61. - PubMed
-
- Wallander J, Ewald U, Lackgren G, Tufveson G, Wahlberg J, Meurling S. Extreme short bowel syndrome in neonates: an indication for small bowel transplantation? Transplant Proc. 1992 Jun;24:1230–5. - PubMed
-
- DeLegge M, Alsolaiman MM, Barbour E, Bassas S, Siddiqi MF, Moore NM. Short bowel syndrome: parenteral nutrition versus intestinal transplantation. Where are we today? Dig Dis Sci. 2007 Apr;52:876–92. - PubMed
-
- Schalamon J, Mayr JM, Hollwarth ME. Mortality and economics in short bowel syndrome. Best Pract Res Clin Gastroenterol. 2003 Dec;17:931–42. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
