

Gadoxetic acid-enhanced T1-weighted MR cholangiography in primary sclerosing cholangitis
- PMID: 22581411
- PMCID: PMC3419782
- DOI: 10.1002/jmri.23683
Gadoxetic acid-enhanced T1-weighted MR cholangiography in primary sclerosing cholangitis
Abstract
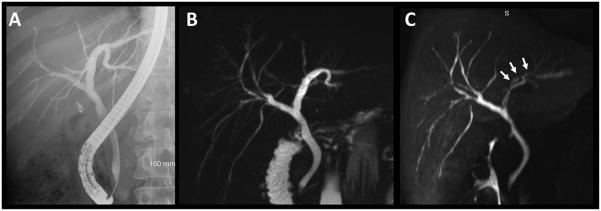
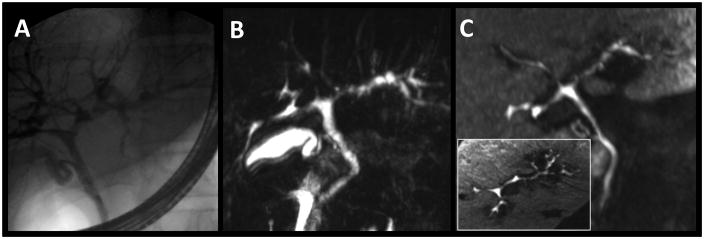
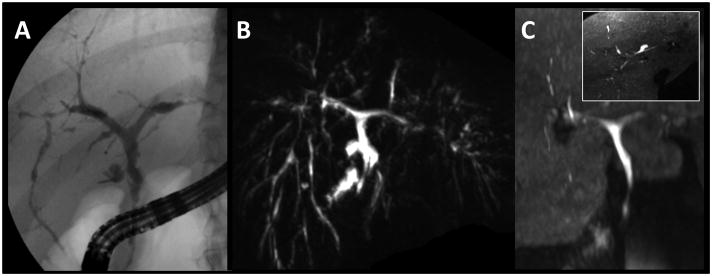
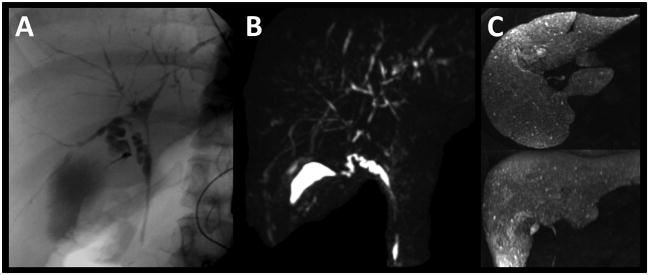
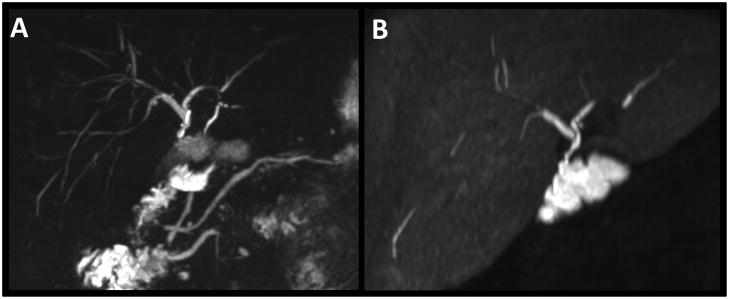
Purpose: To investigate the value of gadoxetic acid-enhanced three-dimensional T1-weighted MR cholangiography (T1w-MRC) in comparison to three-dimensional T2-weighted MR cholangiopancreaticography (T2w-MRCP) in patients with primary sclerosing cholangitis (PSC).
Materials and methods: Thirty-four MR exams in 29 patients (46.0 ± 16.1 years; 19 men, 10 women) scanned within a 14-month period were retrospectively included. Two abdominal radiologists independently evaluated image quality regarding image contrast, image quality degradation due to artifacts, and visualization quality of ducts. The order of biliary tree branches that were visualized and reader preference toward each method were recorded. Helpfulness of T1w-MRC was scored in consensus. Confirmatory endoscopic retrograde cholangiopancreaticography (ERCP) performed within 3 months of the MR examination was available in 8 patients.
Results: Image quality of T1w-MRC and T2w-MRCP was graded good to excellent in all cases. There were advantages for both T1w-MRC (functional information, less degradation due to artifacts) and T2w-MRCP (higher order of visualized branches, better branch depiction). Both readers showed preference for T2w-MRCP; however, both readers found gadoxetic acid-enhanced T1w-MRC helpful in the majority of cases.
Conclusion: Gadoxetic acid-enhanced T1w-MRC is complementary to, but should not replace, T2w-MRCP. T1w-MRC is a useful adjunct to T2w-MRCP for morphologic evaluation and provides additional diagnostic information.
Copyright © 2012 Wiley Periodicals, Inc.
Figures
Similar articles
-
Diagnostic workup of primary sclerosing cholangitis: the benefit of adding gadoxetic acid-enhanced T1-weighted magnetic resonance cholangiography to conventional T2-weighted magnetic resonance cholangiography.Clin Radiol. 2014 May;69(5):499-508. doi: 10.1016/j.crad.2013.12.008. Epub 2014 Mar 12. Clin Radiol. 2014. PMID: 24630133
-
Added value of gadoxetic acid-enhanced T1-weighted magnetic resonance cholangiography for the diagnosis of post-transplant biliary complications.Eur Radiol. 2017 Oct;27(10):4415-4425. doi: 10.1007/s00330-017-4797-9. Epub 2017 Apr 13. Eur Radiol. 2017. PMID: 28409358 Free PMC article.
-
Assessment of biliary anatomy in potential living liver donors: Added value of gadoxetic acid-enhanced T1 MR Cholangiography (MRC) including utilization of controlled aliasing in parallel imaging results in higher acceleration (CAIPIRINHA) technique in comparison to T2W-MRC.Magn Reson Imaging. 2020 Jul;70:64-72. doi: 10.1016/j.mri.2020.04.011. Epub 2020 Apr 19. Magn Reson Imaging. 2020. PMID: 32320722
-
CT and MR cholangiography: advantages and pitfalls in perioperative evaluation of biliary tree.Br J Radiol. 2012 Jul;85(1015):887-96. doi: 10.1259/bjr/21209407. Epub 2012 Mar 14. Br J Radiol. 2012. PMID: 22422383 Free PMC article. Review.
-
MRI of oriental cholangiohepatitis.Clin Radiol. 2011 Feb;66(2):158-63. doi: 10.1016/j.crad.2010.06.017. Epub 2010 Oct 15. Clin Radiol. 2011. PMID: 21216332 Review.
Cited by
-
Diagnosis of functional strictures in patients with primary sclerosing cholangitis using hepatobiliary contrast-enhanced MRI: a proof-of-concept study.Eur Radiol. 2023 Dec;33(12):9022-9037. doi: 10.1007/s00330-023-09915-3. Epub 2023 Jul 20. Eur Radiol. 2023. PMID: 37470827 Free PMC article.
-
Comparison of different magnetic resonance cholangiography techniques in living liver donors including Gd-EOB-DTPA enhanced T1-weighted sequences.PLoS One. 2014 Nov 26;9(11):e113882. doi: 10.1371/journal.pone.0113882. eCollection 2014. PLoS One. 2014. PMID: 25426932 Free PMC article.
-
Clinical guidelines for primary sclerosing cholangitis 2017.J Gastroenterol. 2018 Sep;53(9):1006-1034. doi: 10.1007/s00535-018-1484-9. Epub 2018 Jun 27. J Gastroenterol. 2018. PMID: 29951926 Free PMC article.
-
An Investigation of Transient Severe Motion Related to Gadoxetic Acid-enhanced MR Imaging.Radiology. 2016 Apr;279(1):93-102. doi: 10.1148/radiol.2015150642. Epub 2015 Oct 16. Radiology. 2016. PMID: 26473642 Free PMC article.
-
Primary Sclerosing Cholangitis: Diagnostic Criteria.Tomography. 2024 Jan 7;10(1):47-65. doi: 10.3390/tomography10010005. Tomography. 2024. PMID: 38250951 Free PMC article. Review.
References
-
- Lee YM, Kaplan MM. Primary sclerosing cholangitis. N Engl J Med. 1995;332(14):924–933. - PubMed
-
- Levy C, Lindor KD. Primary sclerosing cholangitis: epidemiology, natural history, and prognosis. Semin Liver Dis. 2006;26(1):22–30. - PubMed
-
- Vitellas KM, El-Dieb A, Vaswani KK, et al. MR cholangiopancreatography in patients with primary sclerosing cholangitis: interobserver variability and comparison with endoscopic retrograde cholangiopancreatography. AJR Am J Roentgenol. 2002;179(2):399–407. - PubMed
-
- Dave M, Elmunzer BJ, Dwamena BA, Higgins PD. Primary sclerosing cholangitis: meta-analysis of diagnostic performance of MR cholangiopancreatography. Radiology. 2010;256(2):387–396. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
