

Urinary spot albumin:creatinine ratio for documenting proteinuria in women with preeclampsia
- PMID: 22582122
- PMCID: PMC3349919
Urinary spot albumin:creatinine ratio for documenting proteinuria in women with preeclampsia
Abstract
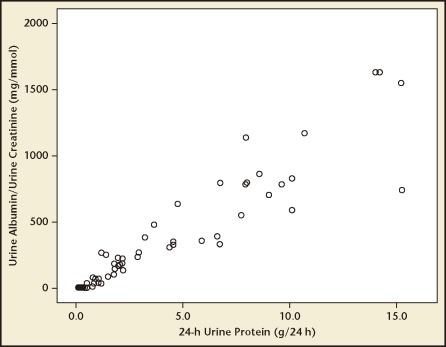
Aim: To assess whether a single urinary spot urinary albumin:creatinine ratio (ACR) can be used to estimate 24-hour urinary protein excretion in women with preeclampsia.
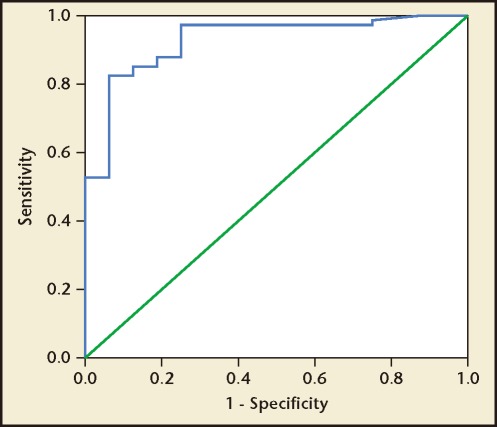
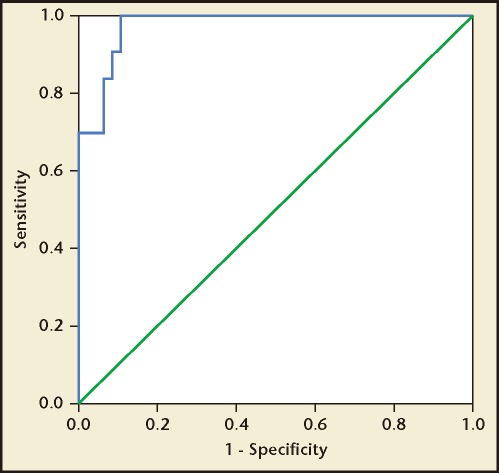
Methods: ACR and 24-hour urinary protein excretion were measured in 50 consecutive patients with preeclampsia. ACR was determined in a spot midstream urine sample and the amount of protein excretion was quantified in a 24-hour urine collection performed the following day. The correlation between the spot ACR and 24-hour urine protein excretion was assessed, and the diagnostic value of ACR was expressed in terms of specificity and sensitivity. Receiver operating characteristic curve analysis was used to determine the best cutoff values of the spot ACR for mild preeclampsia (proteinuria ≥ 0.3 g/24 h) and severe preeclampsia (defined in China as proteinuria ≥ 2 g/24 h).
Results: A strong correlation was evident between the spot ACR and 24-hour urinary protein excretion (r = .938; P < .001). The optimal spot ACR cutoff point was 22.8 mg/mmol for 0.3 g/24 h of protein excretion (mild preeclampsia) with a sensitivity and specificity of 82.4% and 99.4%, respectively, and 155.6 mg/mmol for 2 g/24 h of protein excretion (severe preeclampsia) with a sensitivity and specificity of 90.6% and 99.6%, respectively.
Conclusions: Compared with 24-hour urinary protein excretion, the spot urinary ACR may be a simple, convenient, and accurate indicator of significant proteinuria in women with preeclampsia.
Keywords: Preeclampsia; Proteinuria; Urinary albumin:creatinine ratio.
Figures
References
-
- Martin JA, Hamilton BE, Sutton PD, et al. Births: final data for 2008. Natl Vital Stat Rep. 2010;59:1. - PubMed
-
- Khan KS, Wojdyla D, Say L, et al. WHO analysis of causes of maternal death: a systematic review. Lancet. 2006;367:1066–1074. - PubMed
-
- Lowe SA, Brown MA, Dekker GA, et al. Society of Obstetric Medicine of Australia and New Zealand. Guidelines for the management of hypertensive disorders of pregnancy 2008. Aust N Z J Obstet Gynaecol. 2009;49:242–246. - PubMed
-
- Magee LA, Helewa M, Moutquin JM, von Dadelszen P. Hypertension Guideline Committee; Strategic Training Initiative in Research in the Reproductive Health Sciences (STIRRHS) Scholars. Diagnosis, evaluation, and management of the hypertensive disorders of pregnancy. J Obstet Gynaecol Can. 2008;3(suppl 3):S1–S48. - PubMed
-
- Lindheimer MD, Taler SJ, Cunningham FG. Hypertension in pregnancy. J Am Soc Hypertens. 2008;2:484–494. - PubMed
LinkOut - more resources
Full Text Sources