

Calpain inhibition preserves talin and attenuates right heart failure in acute pulmonary hypertension
- PMID: 22582173
- PMCID: PMC3488694
- DOI: 10.1165/rcmb.2011-0286OC
Calpain inhibition preserves talin and attenuates right heart failure in acute pulmonary hypertension
Abstract
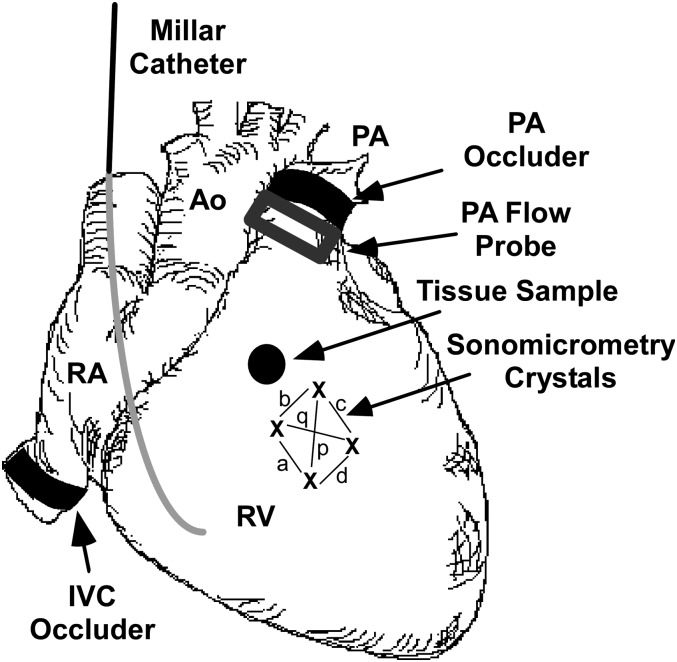
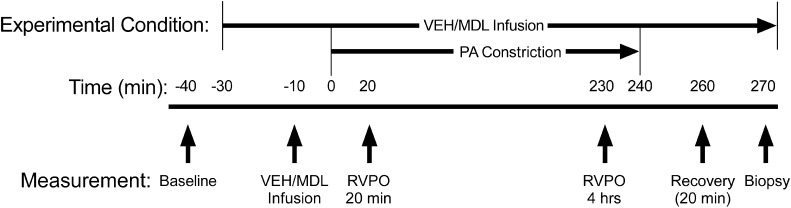
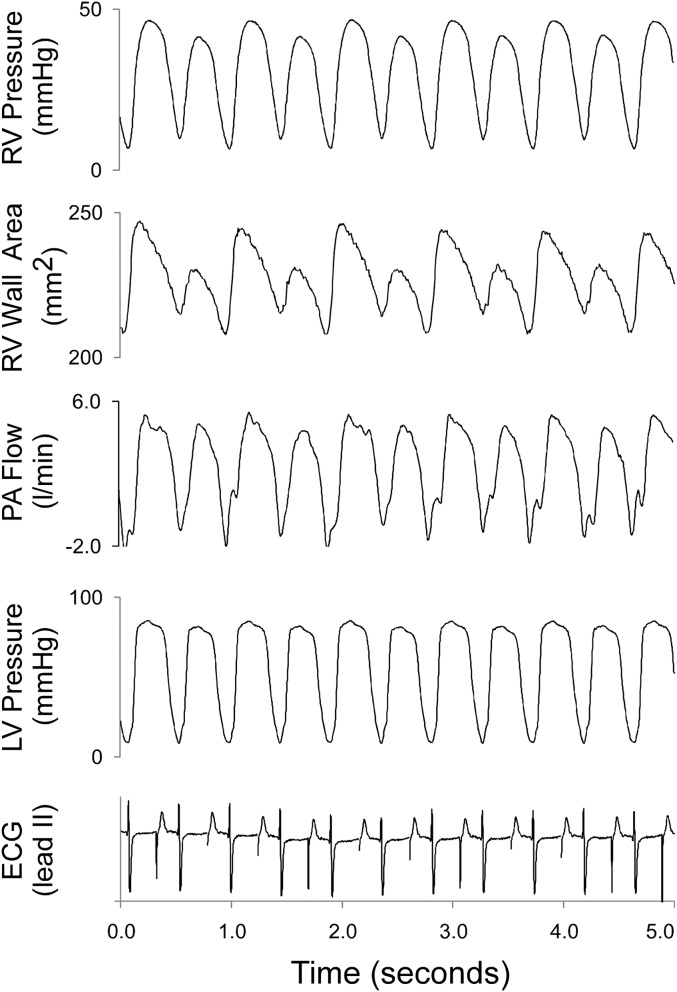
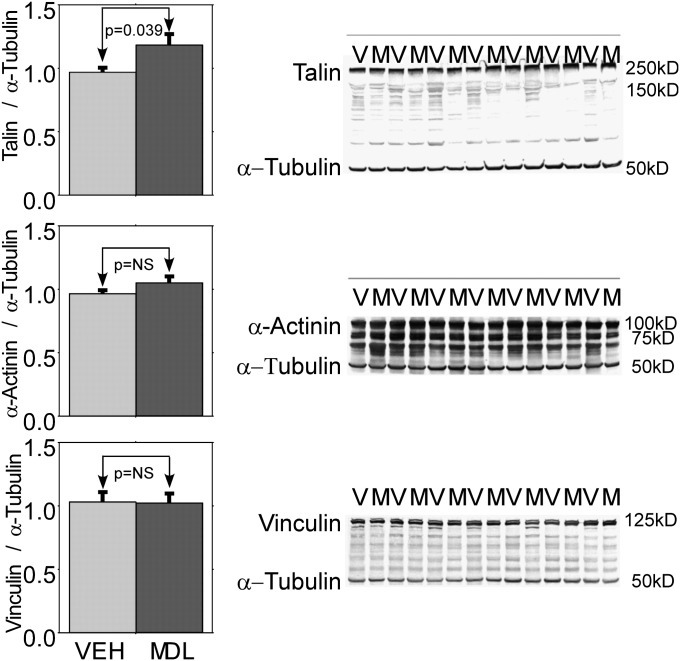
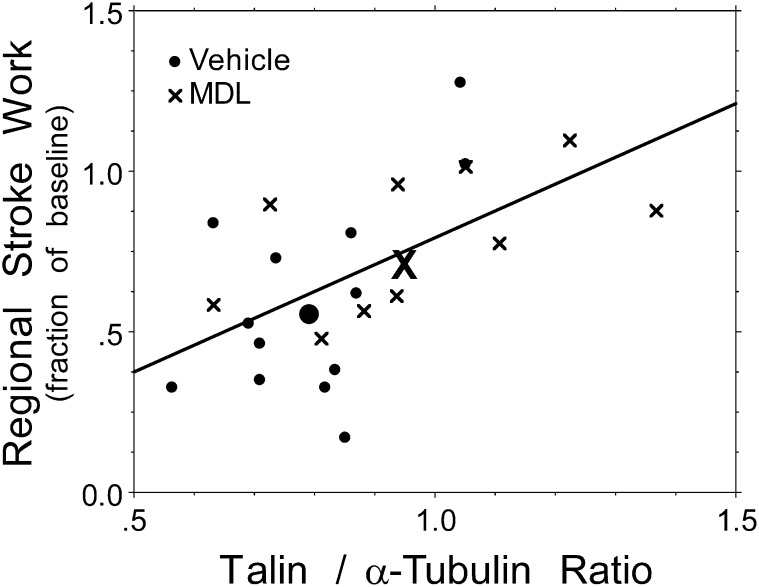
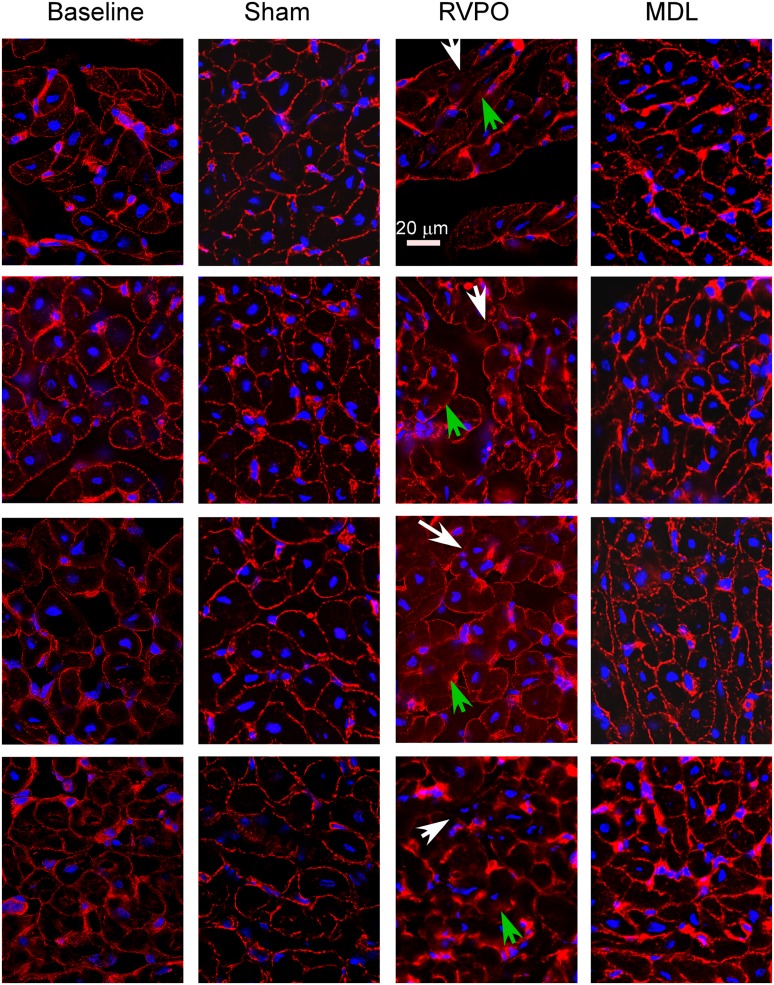
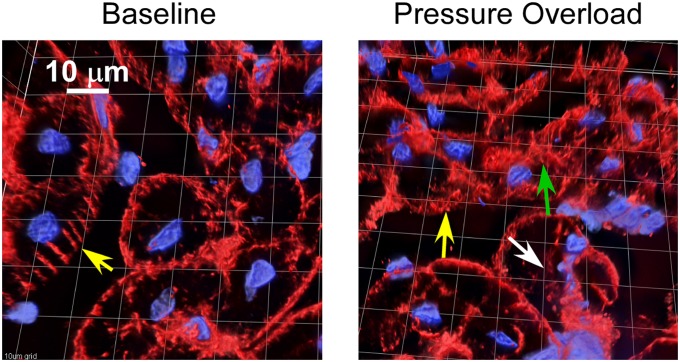
Right heart failure from right ventricular (RV) pressure overload is a major cause of morbidity and mortality, but its mechanism is incompletely understood. We tested the hypothesis that right heart failure during 4 hours of RV pressure overload is associated with alterations of the focal adhesion protein talin, and that the inhibition of calpain attenuates RV dysfunction and preserves RV talin. Anesthetized open-chest pigs treated with the calpain inhibitor MDL-28170 (n = 20) or inactive vehicle (n = 23) underwent 4 hours of RV pressure overload by pulmonary artery constriction (initial RV systolic pressure, 64 ± 1 and 66 ± 1 mm Hg in MDL-28170 and vehicle-treated pigs, respectively). Progressive RV contractile dysfunction was attenuated by MDL-28170: after 4 hours of RV pressure overload, RV systolic pressure was 44 ± 4 mm Hg versus 49 ± 6 mm Hg (P = 0.011), and RV stroke work was 72 ± 5% of baseline versus 90 ± 5% of baseline, (P = 0.027), in vehicle-treated versus MDL-28170-treated pigs, respectively. MDL-28170 reduced the incidence of hemodynamic instability (death or systolic blood pressure of < 85 mm Hg) by 46% (P = 0.013). RV pressure overload disrupted talin organization. MDL-28170 preserved talin abundance in the RV free wall (P = 0.039), and talin abundance correlated with the maintenance of RV free wall stroke work (r = 0.58, P = 0.0039). α-actinin and vinculin showed similar changes according to immunohistology. Right heart failure from acute RV pressure overload is associated with reduced talin abundance and disrupted talin organization. Calpain inhibition preserves the abundance and organization of talin and RV function. Calpain inhibition may offer clinical utility in treating acute cor pulmonale.
Figures
References
-
- Dell’Italia LJ. The right ventricle: anatomy, physiology, and clinical importance. Curr Probl Cardiol 1991;16:653–720 - PubMed
-
- Stobierska-Dzierzek B, Awad H, Michler RE. The evolving management of acute right-sided heart failure in cardiac transplant recipients. J Am Coll Cardiol 2001;38:923–931 - PubMed
-
- Greyson C, Xu Y, Cohen J, Schwartz GG. Right ventricular dysfunction persists following brief right ventricular pressure overload. Cardiovasc Res 1997;34:281–288 - PubMed
-
- Kerbaul F, Rondelet B, Motte S, Fesler P, Hubloue I, Ewalenko P, Naeije R, Brimioulle S. Effects of norepinephrine and dobutamine on pressure load–induced right ventricular failure. Crit Care Med 2004;32:1035–1040 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
