

An improved model for predicting postoperative nausea and vomiting in ambulatory surgery patients using physician-modifiable risk factors
- PMID: 22582204
- PMCID: PMC3534465
- DOI: 10.1136/amiajnl-2012-000872
An improved model for predicting postoperative nausea and vomiting in ambulatory surgery patients using physician-modifiable risk factors
Abstract
Objective: Postoperative nausea and vomiting (PONV) is a frequent complication in patients undergoing ambulatory surgery, with an incidence of 20%-65%. A predictive model can be utilized for decision support and feedback for practitioner practice improvement. The goal of this study was to develop a better model to predict the patient's risk for PONV by incorporating both non-modifiable patient characteristics and modifiable practitioner-specific anesthetic practices.
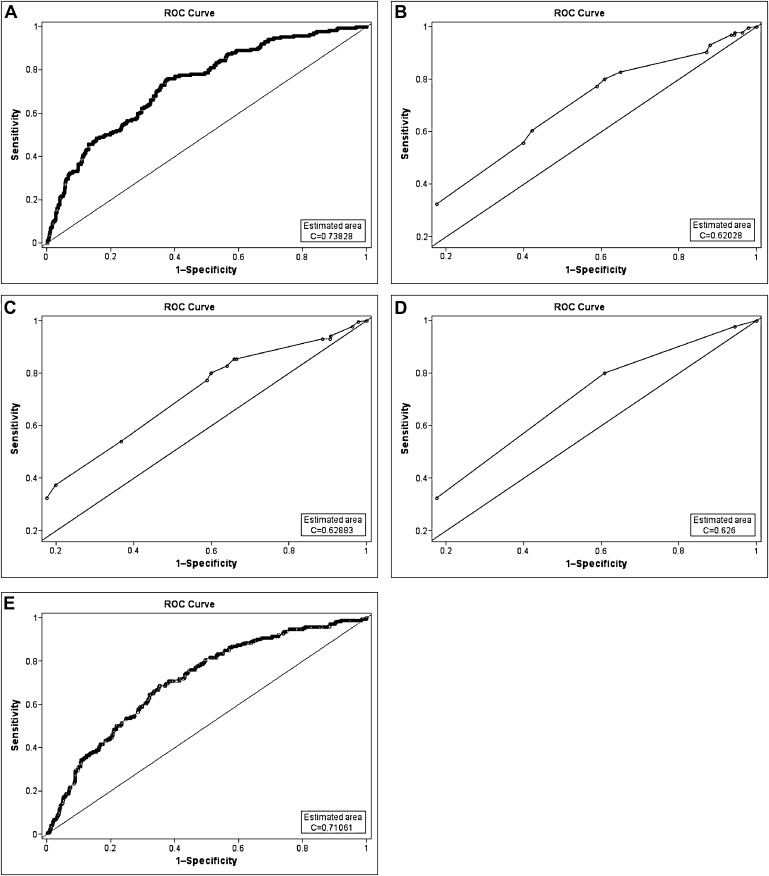
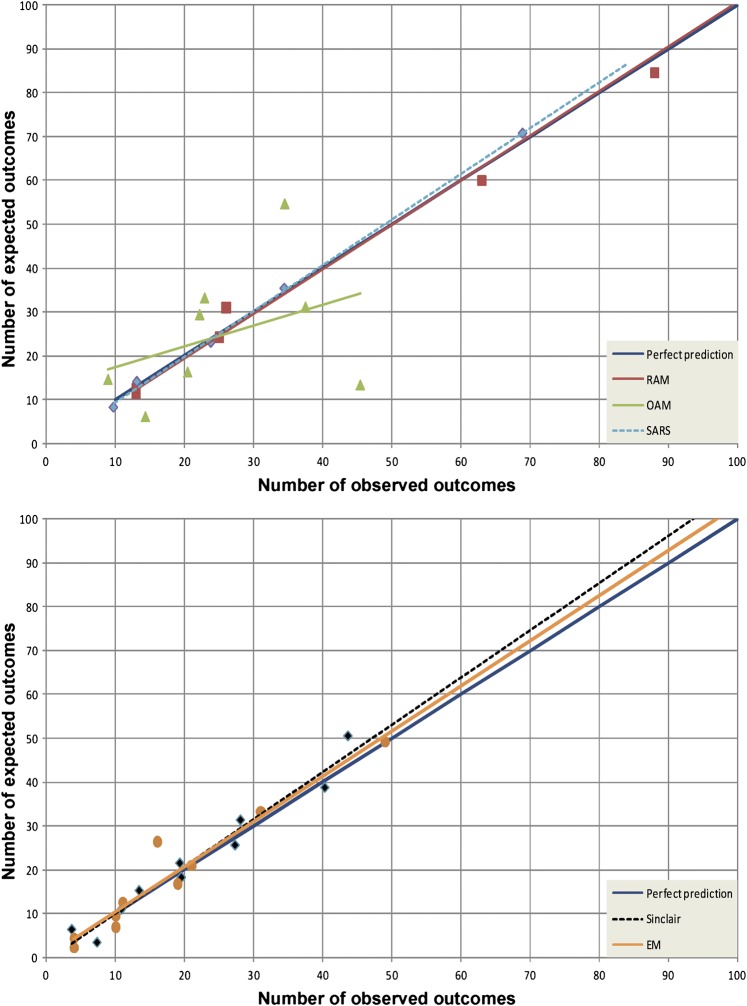
Materials and methods: Data on 2505 ambulatory surgery cases were prospectively collected at an academic center. Sixteen patient-related, surgical, and anesthetic predictors were used to develop a logistic regression model. The experimental model (EM) was compared against the original Apfel model (OAM), refitted Apfel model (RAM), simplified Apfel risk score (SARS), and refitted Sinclair model (RSM) by examining the discriminating power calculated using area under the curve (AUC) and by examining calibration curves.
Results: The EM contained 11 input variables. The AUC was 0.738 for the EM, 0.620 for the OAM, 0.629 for the RAM, 0.626 for the SARS, and 0.711 for the RSM. Pair-wise discrimination comparison of models showed statistically significant differences (p<0.05) in AUC between the EM and all other models, OAM and RSM, RAM and RSM, and SARS and RSM.
Discussion: All models except the OAM appeared to have good calibration for our institution's ambulatory surgery data. Ours is the first model to break down risk by anesthetic technique and incorporate risk reduction due to PONV prophylaxis.
Conclusion: The EM showed statistically significant improved discrimination over existing models and good calibration. However, the EM should be validated at another institution.
Conflict of interest statement
Figures
References
-
- Gan T, Sloan F, Dear Gde L, et al. How much are patients willing to pay to avoid postoperative nausea and vomiting? Anesth Analg 2001;92:393–400 - PubMed
-
- Habib AS, Gan TJ. Evidence-based management of postoperative nausea and vomiting: a review. Can J Anaesth 2004;51:326–41 - PubMed
-
- Palazzo MG, Strunin L. Anaesthesia and emesis. I: Etiology. Can Anaesth Soc J 1984;31:178–87 - PubMed
-
- Watcha MF. The cost-effective management of postoperative nausea and vomiting. Anesthesiology 2000;92:931–3 - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
