

Sequential intensification of metformin treatment in type 2 diabetes with liraglutide followed by randomized addition of basal insulin prompted by A1C targets
- PMID: 22584132
- PMCID: PMC3379583
- DOI: 10.2337/dc11-1928
Sequential intensification of metformin treatment in type 2 diabetes with liraglutide followed by randomized addition of basal insulin prompted by A1C targets
Abstract
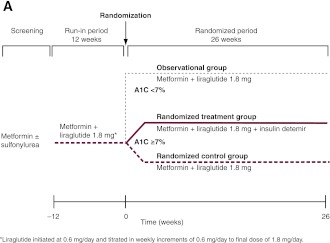
Objective: We evaluated the addition of liraglutide to metformin in type 2 diabetes followed by intensification with basal insulin (detemir) if glycated hemoglobin (A1C) ≥7%.
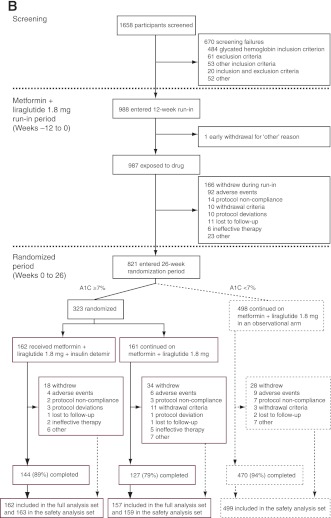
Research design and methods: In 988 participants from North America and Europe uncontrolled on metformin ± sulfonylurea, sulfonylurea was discontinued and liraglutide 1.8 mg/day added for 12 weeks (run-in). Subsequently, those with A1C ≥7% were randomized 1:1 to 26 weeks' open-label addition of insulin detemir to metformin + liraglutide (n = 162) or continuation without insulin detemir (n = 161). Patients achieving A1C <7% continued unchanged treatment (observational arm). The primary end point was A1C change between randomized groups.
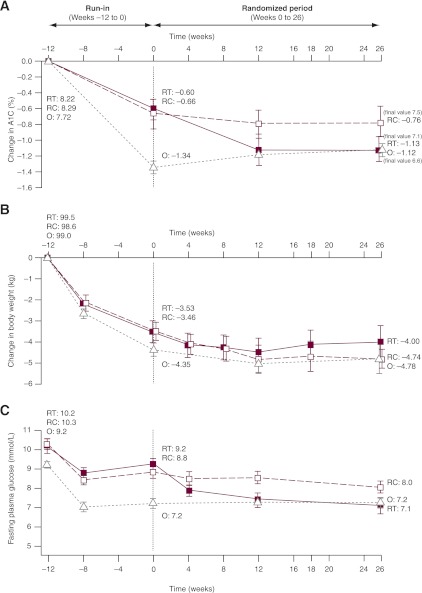
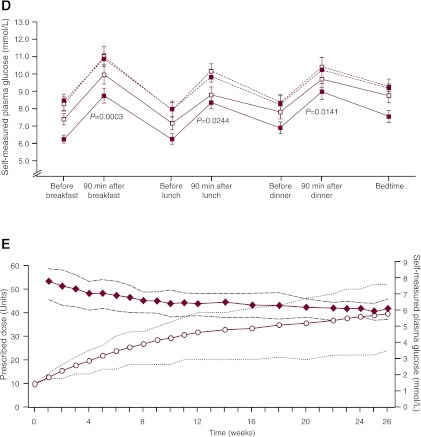
Results: Of 821 participants completing the run-in, 61% (n = 498) achieved A1C <7% (mean change -1.3% from 7.7% at start), whereas 39% (n = 323) did not (-0.6% from 8.3% at start). During run-in, 167 of 988 (17%) withdrew; 46% of these due to gastrointestinal adverse events. At week 26, A1C decreased further, by 0.5% (from 7.6% at randomization) with insulin detemir (n = 162) versus 0.02% increase without insulin detemir (n = 157) to 7.1 and 7.5%, respectively (estimated treatment difference -0.52 [95% CI -0.68 to -0.36]; P < 0.0001). Forty-three percent of participants with insulin detemir versus 17% without reached A1C <7%. Mean weight decreased by 3.5 kg during run-in, then by 0.16 kg with insulin detemir or 0.95 kg without insulin detemir. In the randomized phase, no major hypoglycemia occurred and minor hypoglycemia rates were 0.286 and 0.029 events per participant-year with and without insulin detemir (9.2 vs. 1.3%).
Conclusions: Supplementation of metformin with liraglutide and then insulin detemir was well tolerated in the majority of patients, with good glycemic control, sustained weight loss, and very low hypoglycemia rates.
Trial registration: ClinicalTrials.gov NCT00856986.
Figures
References
-
- Nathan DM, Buse JB, Davidson MB, et al. American Diabetes Association. European Association for the Study of Diabetes Medical management of hyperglycaemia in type 2 diabetes mellitus: a consensus algorithm for the initiation and adjustment of therapy: a consensus statement from the American Diabetes Association and the European Association for the Study of Diabetes. Diabetologia 2009;52:17–30 - PubMed
-
- Buse JB, Rosenstock J, Sesti G, et al. LEAD-6 Study Group Liraglutide once a day versus exenatide twice a day for type 2 diabetes: a 26-week randomised, parallel-group, multinational, open-label trial (LEAD-6). Lancet 2009;374:39–47 - PubMed
-
- Russell-Jones D, Vaag A, Schmitz O, et al. ; Liraglutide Effect and Action in Diabetes 5 (LEAD-5) met+SU Study Group. Liraglutide vs insulin glargine and placebo in combination with metformin and sulfonylurea therapy in type 2 diabetes mellitus (LEAD-5 met+SU): a randomized controlled trial. Diabetologia 2009;52:2046–2055 - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
