

The role of surgeon error in withdrawal of postoperative life support
- PMID: 22584696
- PMCID: PMC3621715
- DOI: 10.1097/SLA.0b013e3182580de5
The role of surgeon error in withdrawal of postoperative life support
Abstract
Background: Surgeons may be reluctant to withdraw postoperative life support after a poor outcome.
Methods: A cross-sectional random sample was taken from a US mail survey of 2100 surgeons who routinely perform high-risk operations. We used a hypothetical vignette of a specialty-specific operation complicated by a hemiplegic stroke and respiratory failure. On postoperative day 7, the patient and family requested withdrawal of life-supporting therapy. We experimentally modified the timing and role of surgeon error to assess their influence on surgeons' willingness to withdraw life-supporting care.
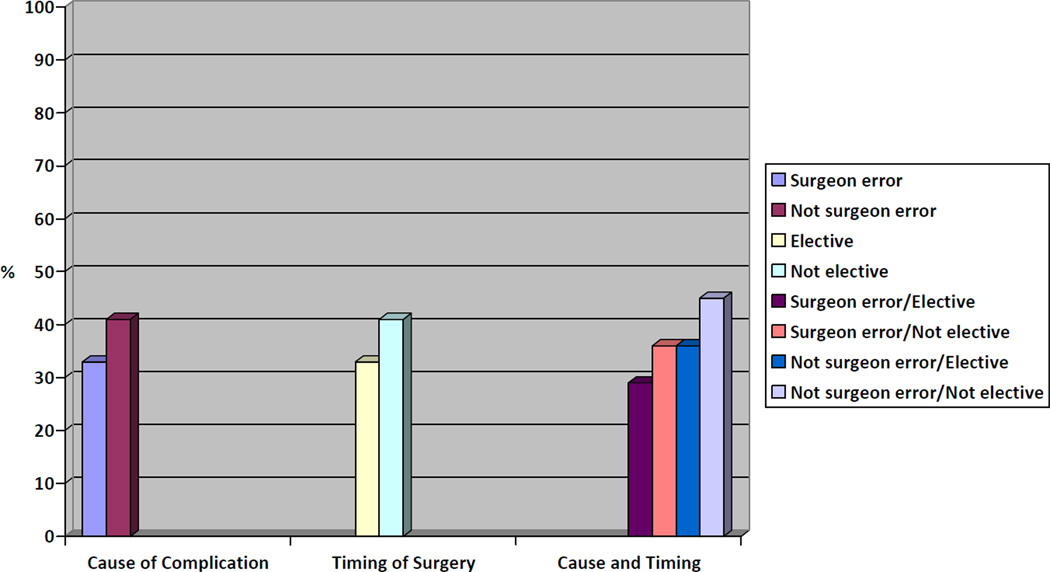
Results: The adjusted response rate was 56%. Sixty-three percent of respondents would not honor the request to withdraw life-supporting treatment. Willingness to withdraw life-support was significantly lower in the setting of surgeon error (33% vs 41%, P < 0.008) and elective operations rather than in emergency cases (33% vs 41%, P = 0.01). After adjustment for specialty, years of experience, geographic region, and gender, odds of withdrawing life-supporting therapy were significantly greater in cases in which the outcome was not explicitly from error during an emergency operation as compared to iatrogenic injury in elective cases (odds ratio 1.95, 95% confidence intervals 1.26-3.01). Surgeons who did not withdraw life-support were significantly more likely to report the importance of optimism regarding prognosis (79% vs 62%, P < 0.0001) and concern that the patient could not accurately predict future quality of life (80% vs 68%, P < 0.0001).
Conclusions: Surgeons are more reluctant to withdraw postoperative life-supporting therapy for patients with complications from surgeon error in the elective setting. This may also be influenced by personal optimism and a belief that patients are unable to predict the value of future health states.
Figures
Comment in
-
Responding to patient requests to withdraw life support: surgical ethics and responsibility.Ann Surg. 2012 Jul;256(1):16-7. doi: 10.1097/SLA.0b013e31825b6a42. Ann Surg. 2012. PMID: 22751516 No abstract available.
References
-
- Bosk CL. Forgive and Remember. Chicago: The University of Chicago Press; 1979. Introduction; pp. 2–34.
-
- Cassell J, Buchman TG, Streat S, Stewart RM. Surgeons, intensivists, and the covenant of care: administrative models and values affecting care at the end of life--Updated. Crit Care Med. 2003;31(5):1551–1557. discussion 7–9. - PubMed
-
- Gerber LA. Transformations in self-understanding in surgeons whose treatment efforts were not successful. Am J Psychother. 1990;44(1):75–84. - PubMed
-
- Burns JP, Edwards J, Johnson J, Cassem NH, Truog RD. Do-not-resuscitate order after 25 years. Crit Care Med. 2003;31(5):1543–1550. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
