

Total parathyroidectomy in a large cohort of cases with hyperparathyroidism associated with multiple endocrine neoplasia type 1: experience from a single academic center
- PMID: 22584718
- PMCID: PMC3328834
- DOI: 10.6061/clinics/2012(sup01)22
Total parathyroidectomy in a large cohort of cases with hyperparathyroidism associated with multiple endocrine neoplasia type 1: experience from a single academic center
Abstract
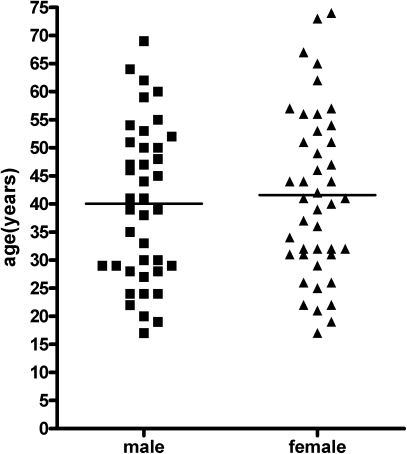
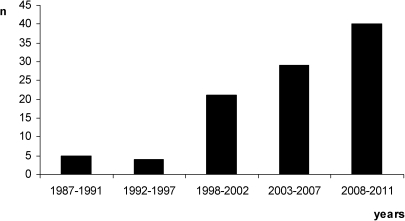
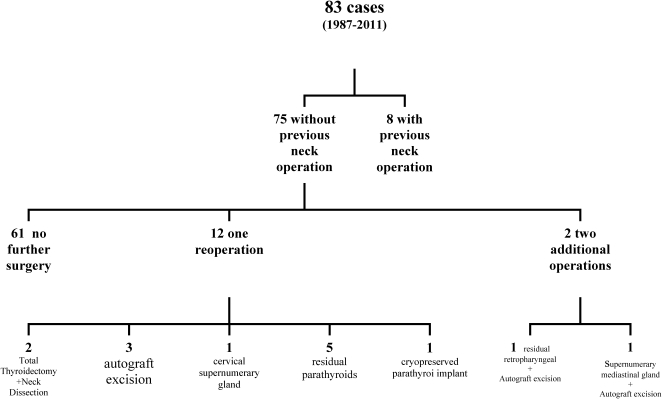
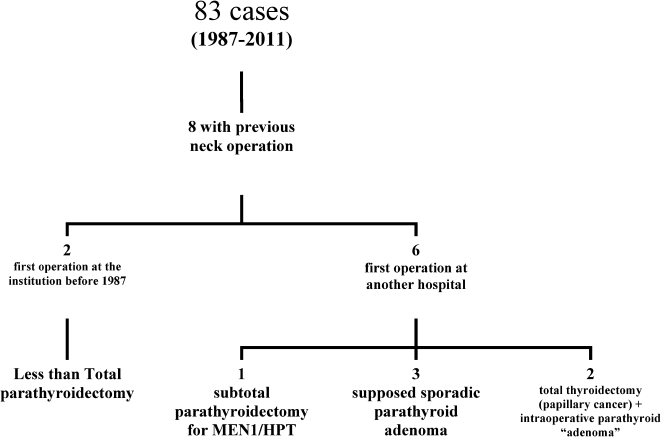
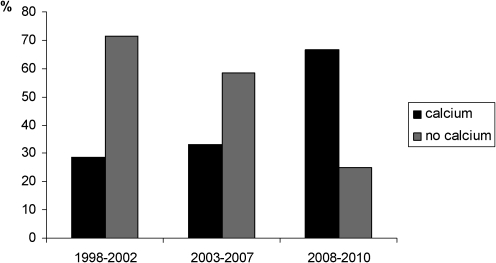
Most cases of sporadic primary hyperparathyroidism present disturbances in a single parathyroid gland and the surgery of choice is adenomectomy. Conversely, hyperparathyroidism associated with multiple endocrine neoplasia type 1 (hyperparathyroidism/multiple endocrine neoplasia type 1) is an asynchronic, asymmetrical multiglandular disease and it is surgically approached by either subtotal parathyroidectomy or total parathyroidectomy followed by parathyroid auto-implant to the forearm. In skilful hands, the efficacy of both approaches is similar and both should be complemented by prophylactic thymectomy. In a single academic center, 83 cases of hyperparathyroidism/ multiple endocrine neoplasia type 1 were operated on from 1987 to 2010 and our first surgical choice was total parathyroidectomy followed by parathyroid auto-implant to the non-dominant forearm and, since 1997, associated transcervical thymectomy to prevent thymic carcinoid. Overall, 40% of patients were given calcium replacement (mean intake 1.6 g/day) during the first months after surgery, and this fell to 28% in patients with longer follow-up. These findings indicate that several months may be needed in order to achieve a proper secretion by the parathyroid auto-implant. Hyperparathyroidism recurrence was observed in up to 15% of cases several years after the initial surgery. Thus, long-term follow-up is recommended for such cases. We conclude that, despite a tendency to subtotal parathyroidectomy worldwide, total parathyroidectomy followed by parathyroid auto-implant is a valid surgical option to treat hyperparathyroidism/multiple endocrine neoplasia type 1. Larger comparative systematic studies are needed to define the best surgical approach to hyperparathyroidism/multiple endocrine neoplasia type 1.
Conflict of interest statement
No potential conflict of interest was reported.
Figures
References
-
- Brandi ML, Gagel RF, Angeli A, Bilezikian JP, Beck-Peccoz P, Bordi C, et al. Guidelines for diagnosis and therapy of MEN type 1 and type 2. J Clin Endocrinol Metab. 2001;86((12)):5658–71. - PubMed
-
- Marx SJ. Molecular genetics of multiple endocrine neoplasia types 1 and 2. Nat Rev Cancer. 2005;5((2)):367–75. - PubMed
-
- Lourenço DM, Jr, Toledo RA, Coutinho FL, Margarido LC, Siqueira SA, dos Santos MA, et al. The impact of clinical and genetic screenings on the management of the multiple endocrine neoplasia type 1. Clinics. 2007;62((4)):465–76. - PubMed
-
- Lips CJM, Dreijerink K, Links TP, Höppener JWM. Multiple endocrine neoplasia type 1. Exp Rev Endocrinol Metab. 2009;4((4)):371–88. - PubMed
-
- Falchetti A, Marini F, Luzi E, Giusti F, Cavalli L, Cavalli T, Brandi ML. Multiple endocrine neoplasia type 1 (MEN1): Not only inherited endocrine tumors. Genet Med. 2009;11((12)):825–35. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
