

Randomized trial of automated, electronic monitoring to facilitate early detection of sepsis in the intensive care unit*
- PMID: 22584763
- PMCID: PMC4451061
- DOI: 10.1097/CCM.0b013e318250a887
Randomized trial of automated, electronic monitoring to facilitate early detection of sepsis in the intensive care unit*
Abstract
Objective: To determine whether automated identification with physician notification of the systemic inflammatory response syndrome in medical intensive care unit patients expedites early administration of new antibiotics or improvement of other patient outcomes in patients with sepsis.
Design: : A prospective randomized, controlled, single center study.
Setting: Medical intensive care unit of an academic, tertiary care medical center.
Patients: Four hundred forty-two consecutive patients admitted over a 4-month period who met modified systemic inflammatory response syndrome criteria in a medical intensive care unit.
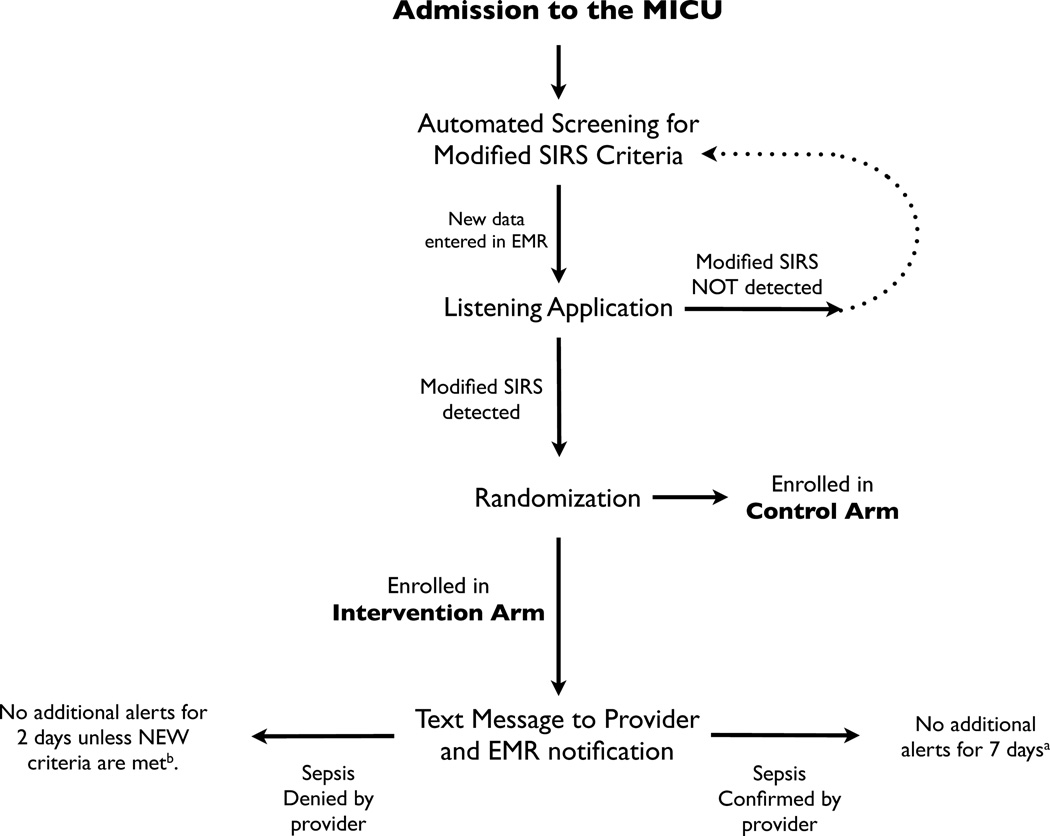
Intervention: Patients were randomized to monitoring by an electronic "Listening Application" to detect modified (systemic inflammatory response syndrome) criteria vs. usual care. The listening application notified physicians in real time when modified systemic inflammatory response syndrome criteria were detected, but did not provide management recommendations.
Measurements and main results: The median time to new antibiotics was similar between the intervention and usual care groups when comparing among all patients (6.0 hr vs. 6.1 hr, p = .95), patients with sepsis (5.3 hr vs. 5.1 hr; p = .90), patients on antibiotics at enrollment (5.2 hr vs. 7.0 hr, p = .27), or patients not on antibiotics at enrollment (5.2 hr vs. 5.1 hr, p = .85). The amount of fluid administered following detection of modified systemic inflammatory response syndrome criteria was similar between groups whether comparing all patients or only patients who were hypotensive at enrollment. Other clinical outcomes including intensive care unit length of stay, hospital length of stay, and mortality were not shown to be different between patients in the intervention and control groups.
Conclusions: Realtime alerts of modified systemic inflammatory response syndrome criteria to physicians in one tertiary care medical intensive care unit were feasible and safe but did not influence measured therapeutic interventions for sepsis or significantly alter clinical outcomes.
Conflict of interest statement
The authors have not disclosed any potential conflicts of interest
Figures
Comment in
-
How can we best use electronic data to find and treat the critically ill?*.Crit Care Med. 2012 Jul;40(7):2242-3. doi: 10.1097/CCM.0b013e318256b99b. Crit Care Med. 2012. PMID: 22710217 No abstract available.
References
-
- Angus DC, Wax RS. Epidemiology of sepsis: an update. Critical Care Medicine. 2001 Jul;29(7 Suppl):S109–S116. - PubMed
-
- Martin GS, Mannino DM, Eaton S, Moss M. The epidemiology of sepsis in the United States from 1979 through 2000. New England Journal of Medicine. 2003 May 17;348(16):1546–1554. - PubMed
-
- Alberti C, Brun-Buisson C, Burchardi H, et al. Epidemiology of sepsis and infection in ICU patients from an international multicentre cohort study. Intensive Care Medicine. 2002 Mar 01;28(2):108–121. - PubMed
-
- Bone R, Balk R, Cerra F, et al. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. The ACCP/SCCM Consensus Conference Committee. American College of Chest Physicians/Society of Critical Care Medicine. Chest. 1992 Jul 01;101(6):1644–1655. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
