

Derivation of a cardiac arrest prediction model using ward vital signs*
- PMID: 22584764
- PMCID: PMC3378796
- DOI: 10.1097/CCM.0b013e318250aa5a
Derivation of a cardiac arrest prediction model using ward vital signs*
Abstract
Objective: Rapid response team activation criteria were created using expert opinion and have demonstrated variable accuracy in previous studies. We developed a cardiac arrest risk triage score to predict cardiac arrest and compared it to the Modified Early Warning Score, a commonly cited rapid response team activation criterion.
Design: A retrospective cohort study.
Setting: An academic medical center in the United States.
Patients: All patients hospitalized from November 2008 to January 2011 who had documented ward vital signs were included in the study. These patients were divided into three cohorts: patients who suffered a cardiac arrest on the wards, patients who had a ward to intensive care unit transfer, and patients who had neither of these outcomes (controls).
Interventions: None.
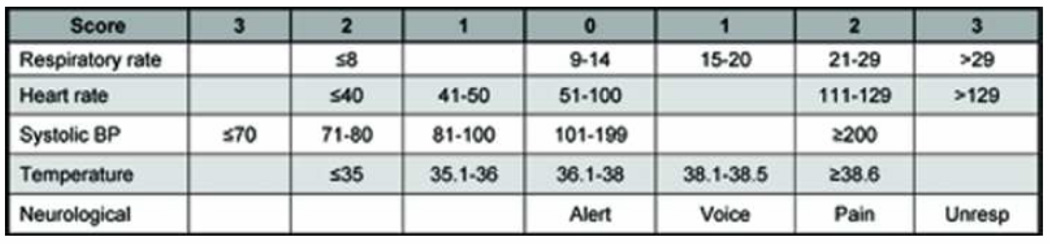
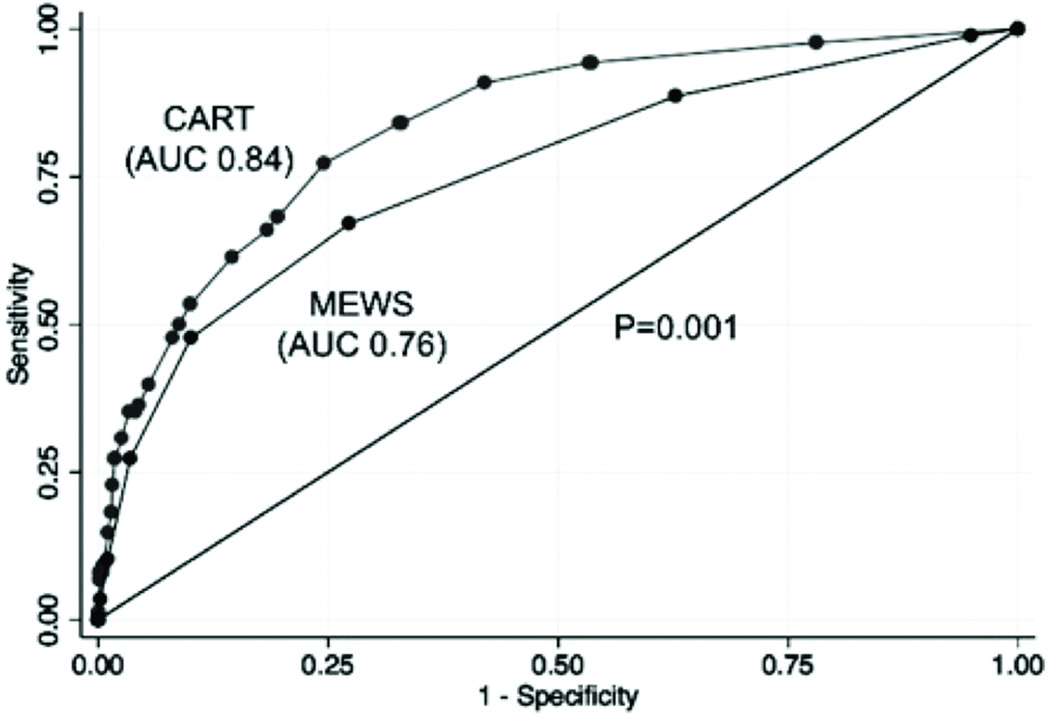
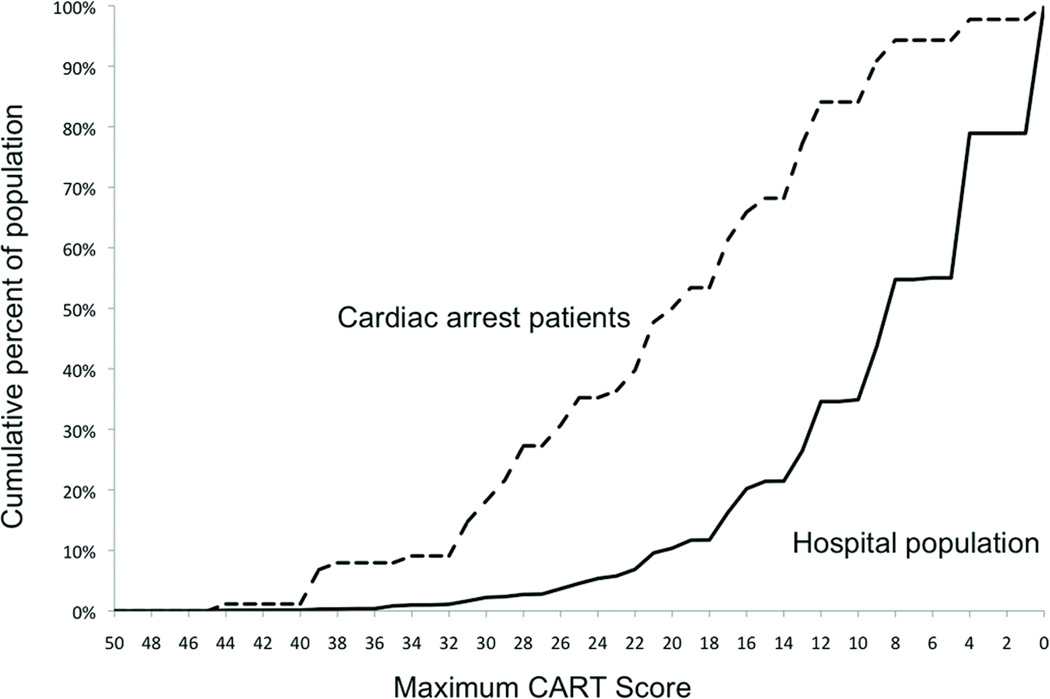
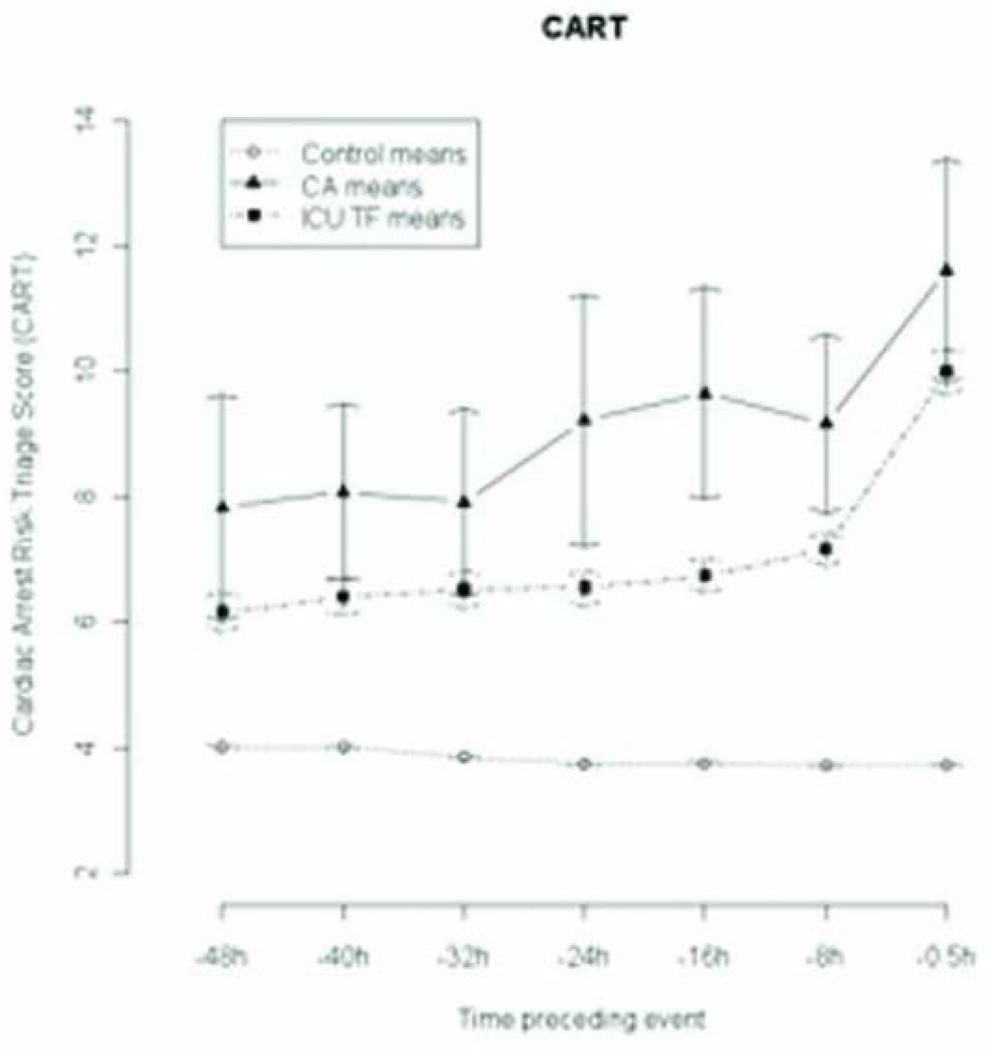
Measurements and main results: Ward vital signs from admission until discharge, intensive care unit transfer, or ward cardiac arrest were extracted from the medical record. Multivariate logistic regression was used to predict cardiac arrest, and the cardiac arrest risk triage score was calculated using the regression coefficients. The model was validated by comparing its accuracy for detecting intensive care unit transfer to the Modified Early Warning Score. Each patient's maximum score prior to cardiac arrest, intensive care unit transfer, or discharge was used to compare the areas under the receiver operating characteristic curves between the two models. Eighty-eight cardiac arrest patients, 2,820 intensive care unit transfers, and 44,519 controls were included in the study. The cardiac arrest risk triage score more accurately predicted cardiac arrest than the Modified Early Warning Score (area under the receiver operating characteristic curve 0.84 vs. 0.76; p = .001). At a specificity of 89.9%, the cardiac arrest risk triage score had a sensitivity of 53.4% compared to 47.7% for the Modified Early Warning Score. The cardiac arrest risk triage score also predicted intensive care unit transfer better than the Modified Early Warning Score (area under the receiver operating characteristic curve 0.71 vs. 0.67; p < .001).
Conclusions: The cardiac arrest risk triage score is simpler and more accurately detected cardiac arrest and intensive care unit transfer than the Modified Early Warning Score. Implementation of this tool may decrease rapid response team resource utilization and provide a better opportunity to improve patient outcomes than the modified early warning score.
Conflict of interest statement
The authors have not disclosed any potential conflicts of interest
Figures
Comment in
-
Identifying the patient at risk of deterioration, intensive care unit admission, or cardiac arrest: stop predicting, start preventing*.Crit Care Med. 2012 Jul;40(7):2243-4. doi: 10.1097/CCM.0b013e3182546875. Crit Care Med. 2012. PMID: 22710218 No abstract available.
References
-
- Peberdy MA, Kaye W, Ornato JP, et al. Cardiopulmonary resuscitation of adults in the hospital: a report of 14720 cardiac arrests from the National Registry of Cardiopulmonary Resuscitation. Resuscitation. 2003;58(3):297–308. - PubMed
-
- Berlot G, Pangher A, Petrucci L, et al. Anticipating events of in-hospital cardiac arrest. Eur J Emerg Med. 2004;11(1):24–28. - PubMed
-
- Sandroni C, Nolan J, Cavallaro F, et al. In-hospital cardiac arrest: incidence, prognosis and possible measures to improve survival. Intensive Care Med. 2007;33(2):237–245. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
