

Impact of changes of positive end-expiratory pressure on functional residual capacity at low tidal volume ventilation during general anesthesia
- PMID: 22584817
- PMCID: PMC3468745
- DOI: 10.1007/s00540-012-1411-9
Impact of changes of positive end-expiratory pressure on functional residual capacity at low tidal volume ventilation during general anesthesia
Abstract
Purpose: Several reports in the literature have described the effects of positive end-expiratory pressure (PEEP) level upon functional residual capacity (FRC) in ventilated patients during general anesthesia. This study compares FRC in mechanically low tidal volume ventilation with different PEEP levels during upper abdominal surgery.
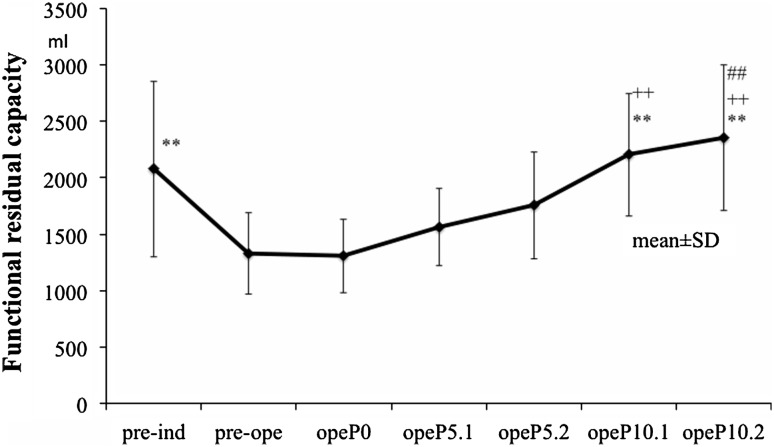
Methods: Before induction of anesthesia (awake) for nine patients with upper abdominal surgery, a tight-seal facemask was applied with 2 cmH(2)O pressure support ventilation and 100 % O(2) during FRC measurements conducted on patients in a supine position. After tracheal intubation, lungs were ventilated with bilevel airway pressure with a volume guarantee (7 ml/kg predicted body weight) and with an inspired oxygen fraction (FIO(2)) of 0.4. PEEP levels of 0, 5, and 10 cmH(2)O were used. Each level of 5 and 10 cmH(2)O PEEP was maintained for 2 h. FRC was measured at each PEEP level.
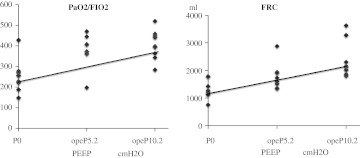
Results: FRC awake was significantly higher than that at PEEP 0 cmH(2)O (P < 0.01). FRC at PEEP 0 cmH(2)O was significantly lower than that at 10 cmH(2)O (P < 0.01). PaO(2)/FIO(2) awake was significantly higher than that for PEEP 0 cmH(2)O (P < 0.01). PaO(2)/FIO(2) at PEEP 0 cmH(2)O was significantly lower than that for PEEP 5 cmH(2)O or PEEP 10 cmH(2)O (P < 0.01). Furthermore, PEEP 0 cmH(2)O, PEEP 5 cmH(2)O after 2 h, and PEEP 10 cmH(2)O after 2 h were correlated with FRC (R = 0.671, P < 0.01) and PaO(2)/FIO(2) (R = 0.642, P < 0.01).
Conclusions: Results suggest that PEEP at 10 cmH(2)O is necessary to maintain lung function if low tidal volume ventilation is used during upper abdominal surgery.
Figures


References
-
- Olegård C, Söndergaard S, Houltz E, Lundin S, Stenqvist O. Estimation of functional residual capacity at the bedside using standard monitoring equipment: a modified nitrogen wash-out/wash-in technique requiring a small change of the inspired oxygen fraction. Anesth Analg. 2005;101:206–212. doi: 10.1213/01.ANE.0000165823.90368.55. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
