

Adherence to antiretroviral therapy and acceptability of planned treatment interruptions in HIV-infected children
- PMID: 22584916
- PMCID: PMC3548111
- DOI: 10.1007/s10461-012-0197-y
Adherence to antiretroviral therapy and acceptability of planned treatment interruptions in HIV-infected children
Abstract
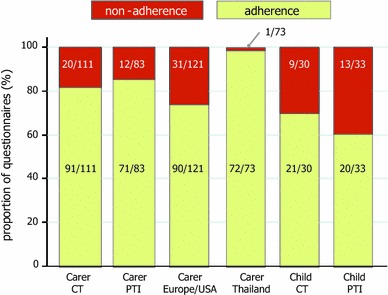
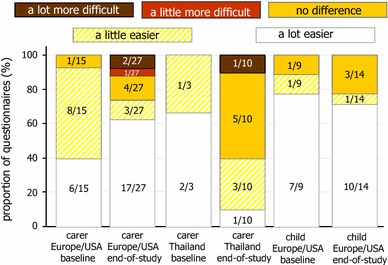
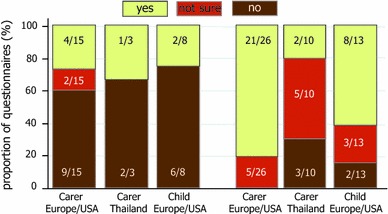
There have been no paediatric randomised trials describing the effect of planned treatment interruptions (PTIs) of antiretroviral therapy (ART) on adherence, or evaluating acceptability of such a strategy. In PENTA 11, HIV-infected children were randomised to CD4-guided PTIs (n = 53) or continuous therapy (CT, n = 56). Carers, and children if appropriate, completed questionnaires on adherence to ART and acceptability of PTIs. There was no difference in reported adherence on ART between CT and PTI groups; non-adherence (reporting missed doses over the last 3 days or marking <100 % adherence since the last clinical visit on a visual analogue scale) was 18 % (20/111) and 14 % (12/83) on carer questionnaires in the CT and PTI groups respectively (odds ratios, OR (95 % CI) = 1.04 (0.20, 5.41), χ(2) (1) = 0.003, p = 0.96). Carers in Europe/USA reported non-adherence more often (31/121, 26 %) than in Thailand (1/73, 1 %; OR (95 % CI) = 54.65 (3.68, 810.55), χ(2) (1) = 8.45, p = 0.004). The majority of families indicated they were happy to have further PTIs (carer: 23/36, 64 %; children: 8/13, 62 %), however many reported more clinic visits during PTI were a problem (carer: 15/36, 42 %; children: 6/12, 50 %).
No ha habido estudios pediátricos randomizados que describan el efecto de las interrupciones planificadas del tratamiento (IPT) antirretroviral en el seguimiento del tratamiento o en la aceptabilidad de dicha estrategia. En PENTA11, niños infectados con HIV fueron randomizados o bien en IPT guiadas por sus CD4 (n = 53) o bien en terapia continua (TC, n = 56). Tanto los cuidadores como los niños, cuando era apropiado, completaron cuestionarios de seguimiento de la terapia antirretroviral y de aceptabilidad de las interrupciones. No se encontró diferencia en cuanto al seguimiento del tratamiento entre los dos grupos. No seguimiento (dosis perdidas durante los últimos 3 días o <100 % desde la ultima visita a la clínica en una escala visual analógica) fue del 18 % (20/111) y del 14 % (12/183) en los cuestionarios de los cuidadores en TC y en IPT respectivamente (odds ratios, OR (95 % CI) = 1.04 (0.20, 5.41), χ2 (1) = 0.003, p = 0.96). Los cuidadores en Europa/USA informaron de un no seguimiento del tratamiento más a menudo (31/121, 26 %) que en Tailandia (1/73, 1%; OR (95 % CI) = 54.65 (3.68, 810.55), χ2 (1) = 8.45, p = 0.004). La mayoría de las familias indicaron que les gustaría realizar más ITP (cuidador: 23/36, 64 %; niños: 8/13, 62 %), sin embargo muchos indicaron que el mayor numero de visitas a la clínica durante la IPT era un problema (cuidador: 15/35, 43 %; niños: 6/12, 50 %).
Figures
References
-
- Judd A, Doerholt K, Tookey PA, Sharland M, Riordan A, Menson E, et al. Morbidity, mortality, and response to treatment by children in the United Kingdom and Ireland with perinatally acquired HIV infection during 1996–2006: planning for teenage and adult care. Clin Infect Dis. 2007;45(7):918–924. doi: 10.1086/521167. - DOI - PubMed
-
- Paterson DL, Swindells S, Mohr J, Brester M, Vergis EN, Squier C, et al. Adherence to protease inhibitor therapy and outcomes in patients with HIV infection. Ann Intern Med. 2000;133(1):21–30. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
