

What are the patterns of injury and displacement seen in lateral compression pelvic fractures?
- PMID: 22585347
- PMCID: PMC3392389
- DOI: 10.1007/s11999-012-2364-x
What are the patterns of injury and displacement seen in lateral compression pelvic fractures?
Abstract
Background: Lateral compression (LC)-type pelvic fractures encompass a wide spectrum of injuries. Current classification systems are poorly suited to help guide treatment and do not adequately describe the wide range of injuries seen in clinical practice.
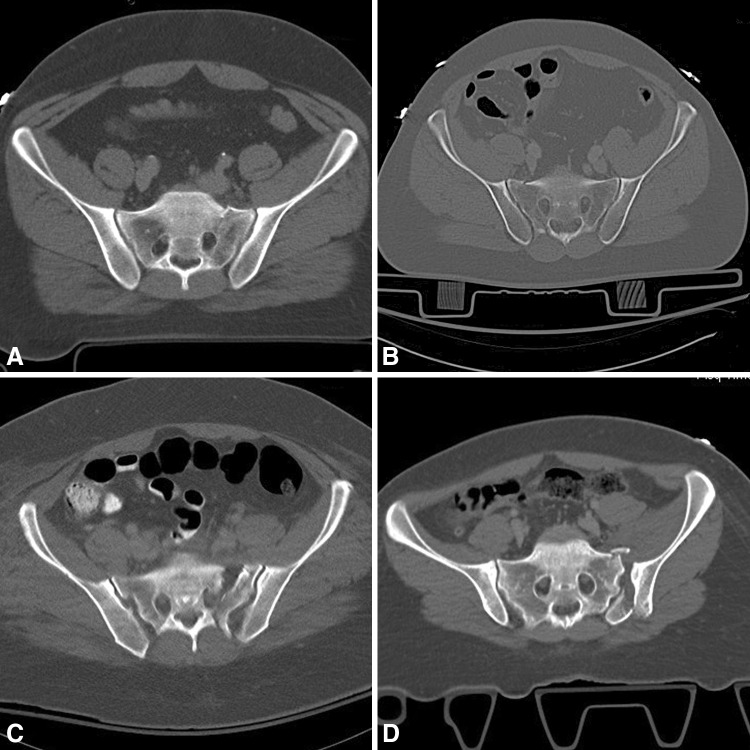
Questions/purposes: We therefore (1) defined the spectrum of injuries that compose LC fractures with respect to both anterior and posterior ring injuries, with particular focus on the morphology of sacral fractures, and (2) identified fracture patterns associated with displacement at presentation.
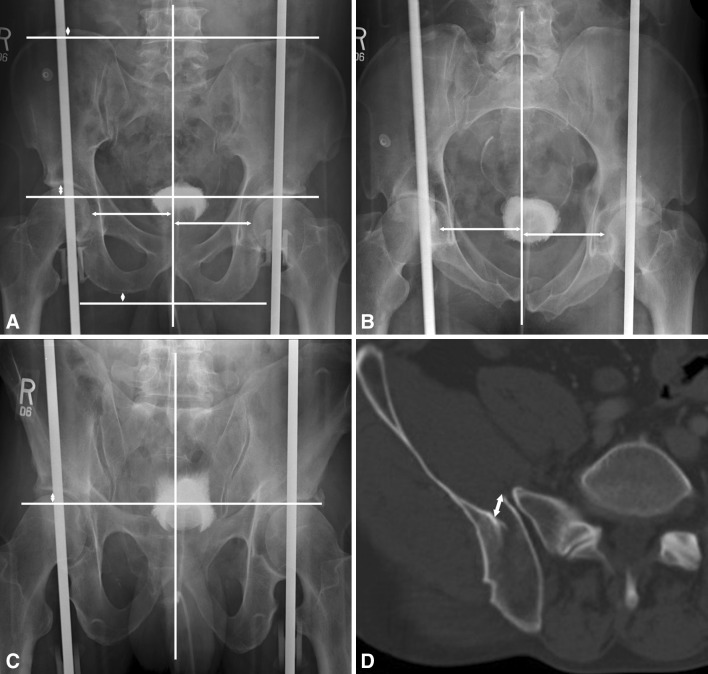
Methods: We retrospectively reviewed 318 LC pelvic fractures. Displacement of the anterior pelvic ring was identified and measured on plain radiographs and posterior displacement was identified by CT.
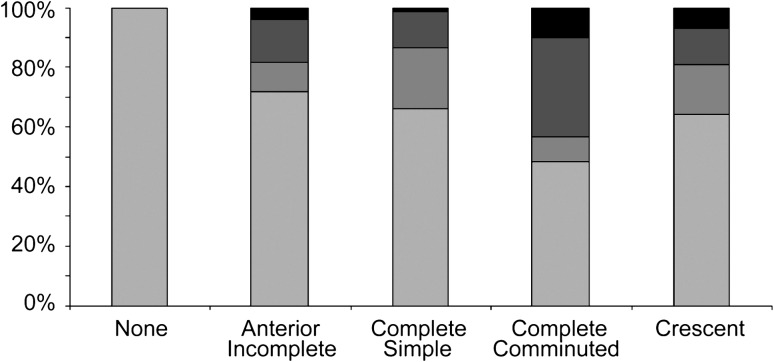
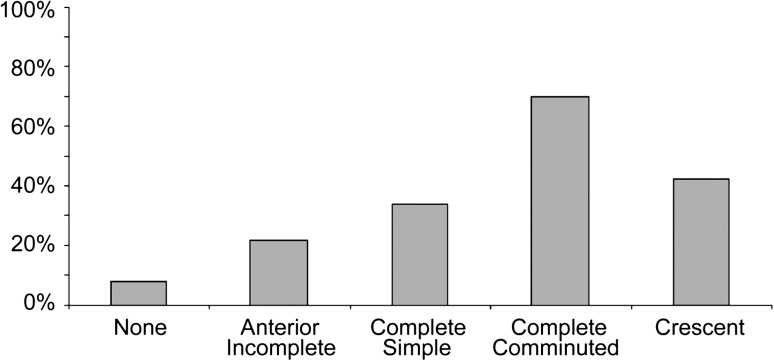
Results: All 318 patients had an anterior injury and all but 13 (4%) had a posterior injury; 263 of the 318 fractures (87%) included a sacral fracture, with 162 of 318 (51%) having an anterior incomplete sacral fracture, 53 (17%) a complete simple fracture, and 48 (15%) a complete comminuted fracture. Forty-two of 318 (13%) had a crescent fracture. One hundred six of 318 (33%) were displaced at presentation. There was a higher incidence of initial displacement observed in fractures including bilateral rami fractures, a comminuted sacral fracture, or a crescent fracture.
Conclusions: LC pelvic fractures represent a heterogeneous group of injuries with a wide range of associated fracture patterns. In particular, there is a wide range of fracture types represented by injuries classified as LC1 (involving any sacral fracture). Fractures with more complex sacral fractures, crescent fractures, or bilateral pubic rami fractures tend to have higher degrees of initial displacement.
Level of evidence: Level IV, diagnostic study. See Instructions for Authors for a complete description of levels of evidence.
Figures
References
-
- Denis F, Davis S, Comfort T. Sacral fractures: an important problem. Retrospective analysis of 236 cases. Clin Orthop Relat Res. 1988;227:67–81. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
