

Pulmonary venous anatomy imaging with low-dose, prospectively ECG-triggered, high-pitch 128-slice dual-source computed tomography
- PMID: 22586259
- PMCID: PMC3384510
- DOI: 10.1161/CIRCEP.111.968313
Pulmonary venous anatomy imaging with low-dose, prospectively ECG-triggered, high-pitch 128-slice dual-source computed tomography
Abstract
Background: The efforts to reduce radiation from cardiac computed tomography (CT) are essential. Using a prospectively triggered, high-pitch dual-source CT protocol, we aim to determine the radiation dose and image quality in patients undergoing pulmonary vein (PV) imaging.
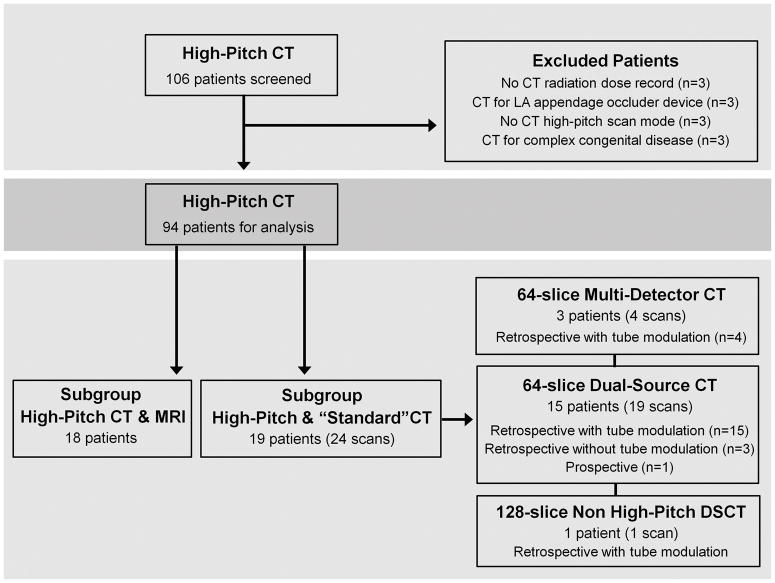
Methods and results: In 94 patients (61±9 years; 71% male) who underwent 128-slice dual-source CT (pitch 3.4), radiation dose and image quality were assessed and compared between 69 patients with sinus rhythm and 25 patients with atrial fibrillation. Radiation dose was compared in a subset of 19 patients with prior retrospective or prospectively triggered CT PV scans without high pitch. In a subset of 18 patients with prior magnetic resonance imaging for PV assessment, PV anatomy and scan duration were compared with high-pitch CT. Using the high-pitch protocol, total effective radiation dose was 1.4 (1.3, 1.9) mSv, with no difference between sinus rhythm and atrial fibrillation (1.4 versus 1.5 mSv; P=0.22). No high-pitch CT scans were nondiagnostic or had poor image quality. Radiation dose was reduced with high-pitch (1.6 mSv) compared with standard protocols (19.3 mSv; P<0.0001). This radiation dose reduction was seen with sinus rhythm (1.5 versus 16.7 mSv; P<0.0001) but was more profound with atrial fibrillation (1.9 versus 27.7 mSv; P=0.039). There was excellent agreement of PV anatomy (κ 0.84; P<0.0001) and a shorter CT scan duration (6 minutes) compared with magnetic resonance imaging (41 minutes; P<0.0001).
Conclusions: Using a high-pitch dual-source CT protocol, PV imaging can be performed with minimal radiation dose, short scan acquisition, and excellent image quality in patients with sinus rhythm or atrial fibrillation. This protocol highlights the success of new cardiac CT technology to minimize radiation exposure, giving clinicians a new low-dose imaging alternative to assess PV anatomy.
Conflict of interest statement
Figures





References
-
- Calkins H, Brugada J, Packer DL, Cappato R, Chen SA, Crijns HJ, Damiano RJ, Jr, Davies DW, Haines DE, Haissaguerre M, Iesaka Y, Jackman W, Jais P, Kottkamp H, Kuck KH, Lindsay BD, Marchlinski FE, McCarthy PM, Mont JL, Morady F, Nademanee K, Natale A, Pappone C, Prystowsky E, Raviele A, Ruskin JN, Shemin RJ. HRS/EHRA/ECAS expert consensus statement on catheter and surgical ablation of atrial fibrillation: recommendations for personnel, policy, procedures and follow-up. A report of the Heart Rhythm Society (HRS) Task Force on Catheter and Surgical Ablation of Atrial Fibrillation developed in partnership with the European Heart Rhythm Association (EHRA) and the European Cardiac Arrhythmia Society (ECAS); in collaboration with the American College of Cardiology (ACC), American Heart Association (AHA), and the Society of Thoracic Surgeons (STS). Endorsed and approved by the governing bodies of the American College of Cardiology, the American Heart Association, the European Cardiac Arrhythmia Society, the European Heart Rhythm Association, the Society of Thoracic Surgeons, and the Heart Rhythm Society. Europace. 2007;9:335–379. - PubMed
-
- Lacomis JM, Goitein O, Deible C, Schwartzman D. CT of the pulmonary veins. J Thorac Imaging. 2007;22:63–76. - PubMed
-
- Schwartzman D, Lacomis J, Wigginton WG. Characterization of left atrium and distal pulmonary vein morphology using multidimensional computed tomography. J Am Coll Cardiol. 2003;41:1349–1357. - PubMed
-
- Jongbloed MR, Bax JJ, Lamb HJ, Dirksen MS, Zeppenfeld K, van der Wall EE, de Roos A, Schalij MJ. Multislice computed tomography versus intracardiac echocardiography to evaluate the pulmonary veins before radiofrequency catheter ablation of atrial fibrillation: a head-to-head comparison. J Am Coll Cardiol. 2005;45:343–350. - PubMed
-
- Tops LF, Bax JJ, Zeppenfeld K, Jongbloed MR, Lamb HJ, van der Wall EE, Schalij MJ. Fusion of multislice computed tomography imaging with three-dimensional electroanatomic mapping to guide radiofrequency catheter ablation procedures. Heart Rhythm. 2005;2:1076–1081. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
