

Reliability of two different presurgical preparation methods for implant dentistry based on panoramic radiography and cone-beam computed tomography in cadavers
- PMID: 22586521
- PMCID: PMC3349045
- DOI: 10.5051/jpis.2012.42.2.39
Reliability of two different presurgical preparation methods for implant dentistry based on panoramic radiography and cone-beam computed tomography in cadavers
Abstract
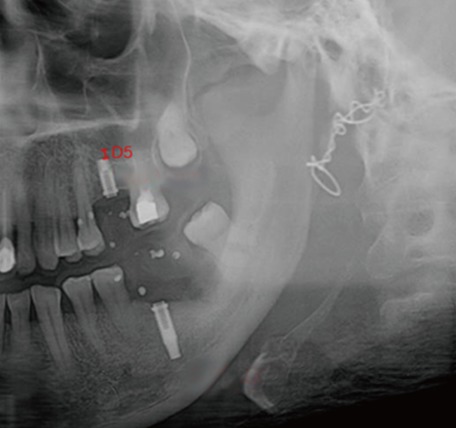
Purpose: Special care is necessary to avoid invading important anatomic structures during surgery when presurgical planning is made based on radiographs. However, none of these types of radiography represents a perfect modality. The purpose of this study was to determine the reliability of presurgical planning based on the use of two types of radiographic image (digital panoramic radiography [DPR] and cone-beam computed tomography [CBCT]) by beginner dentists to place implants, and to quantify differences in measurements between radiographic images and real specimens.
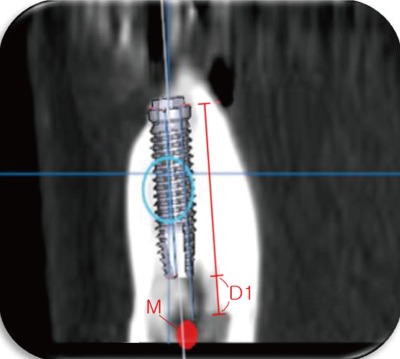
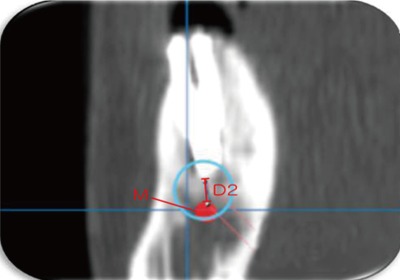
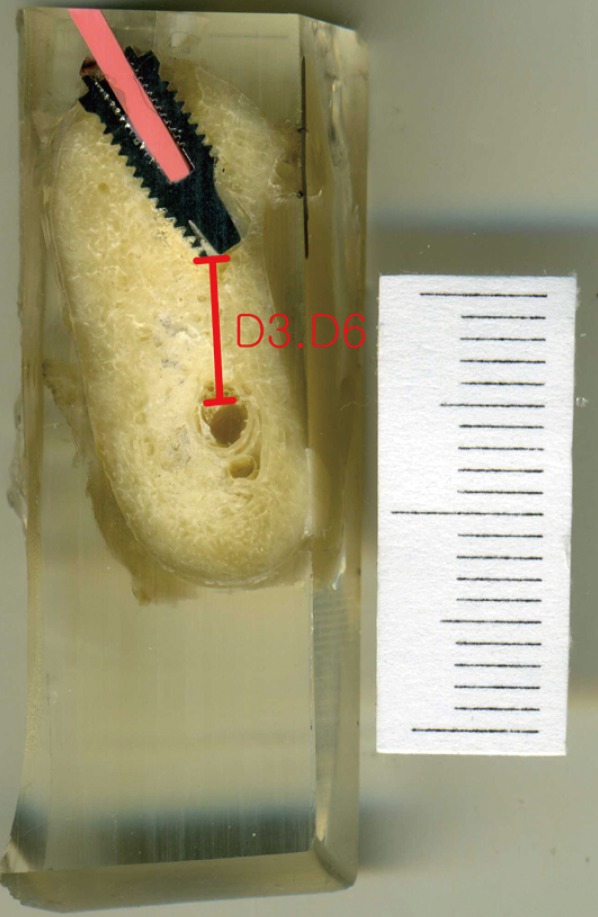
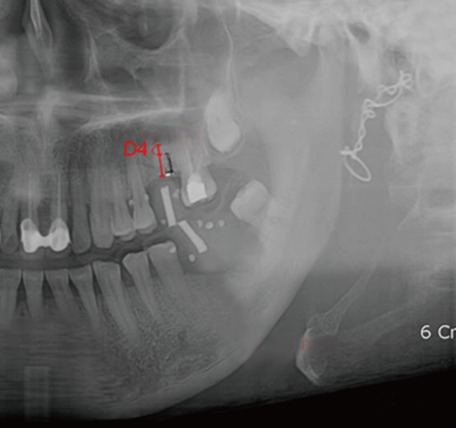
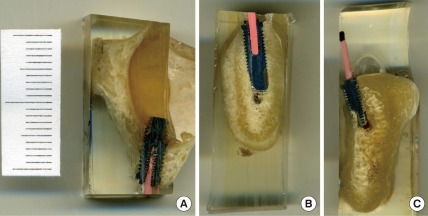
Methods: Ten fresh cadavers without posterior teeth were used, and twelve practitioners who had no experience of implant surgery performed implant surgery after 10 hours of basic instruction using conventional surgical guide based on CBCT or DPR. Two types of measurement error were evaluated: 1) the presurgical measurement error, defined as that between the presurgical and postsurgical measurements in each modality of radiographic analysis, and 2) the measurement error between postsurgical radiography and the real specimen.
Results: The mean presurgical measurement error was significantly smaller for CBCT than for DPR in the maxillary region, whereas it did not differ significantly between the two imaging modalities in the mandibular region. The mean measurement error between radiography and real specimens was significantly smaller for CBCT than for DPR in the maxillary region, but did not differ significantly in the mandibular region.
Conclusions: Presurgical planning can be performed safely using DPR in the mandible; however, presurgical planning using CBCT is recommended in the maxilla when a structure in a buccolingual location needs to be evaluated because this imaging modality supplies buccolingual information that cannot be obtained from DPR.
Keywords: Complications; Cone-beam computed tomography; Dental Implantation; Panoramic radiography.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
Similar articles
-
Comparison between digital panoramic radiography and cone-beam computed tomography for the identification of the mandibular canal as part of presurgical dental implant assessment.J Oral Maxillofac Surg. 2008 Oct;66(10):2130-5. doi: 10.1016/j.joms.2008.06.021. J Oral Maxillofac Surg. 2008. PMID: 18848113
-
Reliability of Orthopantomography and Cone-beam Computed Tomography in Presurgical Implant Planning: A Clinical Study.J Contemp Dent Pract. 2017 Aug 1;18(8):665-669. doi: 10.5005/jp-journals-10024-2103. J Contemp Dent Pract. 2017. PMID: 28816186
-
Radiographic modalities for diagnosis and treatment planning in implant dentistry.Implant Soc. 1995;5(5):7-11. Implant Soc. 1995. PMID: 9571835 Review.
-
Identification and classification of pulp calcifications in posterior teeth according to dental condition using digital panoramic radiography and cone beam CT.Dentomaxillofac Radiol. 2024 Jun 28;53(5):308-315. doi: 10.1093/dmfr/twae015. Dentomaxillofac Radiol. 2024. PMID: 38608191 Free PMC article.
-
Cone beam computed tomography in implant dentistry: recommendations for clinical use.BMC Oral Health. 2018 May 15;18(1):88. doi: 10.1186/s12903-018-0523-5. BMC Oral Health. 2018. PMID: 29764458 Free PMC article. Review.
Cited by
-
Reliability and accuracy of cone-beam computed tomography voxel density and linear distance measurement at different voxel sizes: A study on sheep head cadaver.J Dent Sci. 2017 Jun;12(2):145-150. doi: 10.1016/j.jds.2016.11.004. Epub 2017 Mar 31. J Dent Sci. 2017. PMID: 30895040 Free PMC article.
-
Assessment of the mandibular incisive canal by panoramic radiograph and cone-beam computed tomography.Int J Dent. 2014;2014:187085. doi: 10.1155/2014/187085. Epub 2014 Sep 23. Int J Dent. 2014. PMID: 25332719 Free PMC article.
-
Comparison of the Efficacy of the Panoramic and Cone Beam Computed Tomography Imaging Methods in the Surgical Planning of the Maxillary All-On-4, M-4, and V-4.Biomed Res Int. 2022 Jul 27;2022:1553340. doi: 10.1155/2022/1553340. eCollection 2022. Biomed Res Int. 2022. PMID: 35937385 Free PMC article.
-
Comparison of Dental Panoramic Radiography and CBCT for Measuring Vertical Bone Height in Different Horizontal Locations of Posterior Mandibular Alveolar Process.J Dent (Shiraz). 2018 Jun;19(2):83-91. J Dent (Shiraz). 2018. PMID: 29854881 Free PMC article.
-
Comparing the precision of panoramic radiography and cone-beam computed tomography in avoiding anatomical structures critical to dental implant surgery: A retrospective study.Imaging Sci Dent. 2018 Dec;48(4):269-275. doi: 10.5624/isd.2018.48.4.269. Epub 2018 Dec 20. Imaging Sci Dent. 2018. PMID: 30607351 Free PMC article.
References
-
- Albrektsson T, Dahl E, Enbom L, Engevall S, Engquist B, Eriksson AR, et al. Osseointegrated oral implants: a Swedish multicenter study of 8139 consecutively inserted Nobelpharma implants. J Periodontol. 1988;59:287–296. - PubMed
-
- Misch CE, Perel ML, Wang HL, Sammartino G, Galindo-Moreno P, Trisi P, et al. Implant success, survival, and failure: the International Congress of Oral Implantologists (ICOI) Pisa Consensus Conference. Implant Dent. 2008;17:5–15. - PubMed
-
- Van de Velde T, Glor F, De Bruyn H. A model study on flapless implant placement by clinicians with a different experience level in implant surgery. Clin Oral Implants Res. 2008;19:66–72. - PubMed
-
- Spector L. Computer-aided dental implant planning. Dent Clin North Am. 2008;52:761–775. vi. - PubMed
-
- Hong YH, Mun SK. A case of massive maxillary sinus bleeding after dental implant. Int J Oral Maxillofac Surg. 2011;40:758–760. - PubMed
LinkOut - more resources
Full Text Sources
