

Endosonography in solid and cystic pancreatic tumors
- PMID: 22586537
- PMCID: PMC3350895
- DOI: 10.4161/jig.1.4.19971
Endosonography in solid and cystic pancreatic tumors
Abstract
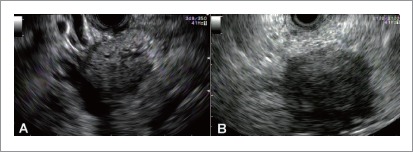
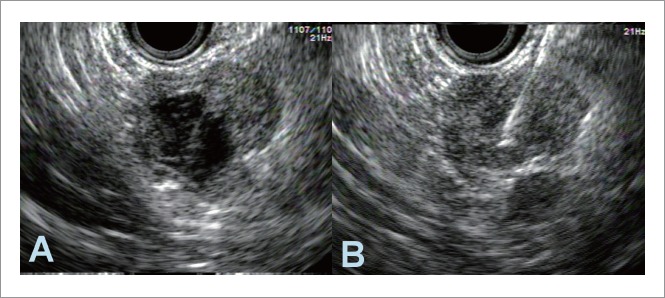
Pancreatic tumors being either benign or malignant can be solid or cystic. Although diverse in presentation, their imaging features share commonalities and it is often difficult to distinguish these tumors. Endoscopic ultrasonography (EUS) is the most sensitive of the imaging procedures currently available for characterizing pancreatic tumors, and is especially good in identifying the smaller sized tumors. Additional applications inclusive of EUS-guided fine needle aspiration (EUS-FNA) are useful in tissue sampling and preoperative staging of pancreatic tumors.Although diagnostic capabilities have greatly evolved with advances in EUS and tissue processing technology (cytology, tumor markers, DNA analysis), differentiation of benign and malignant neoplasms, neoplastic and non-neoplastic (chronic pancreatitis) conditions, continues to be challenging.Recent innovative applications include contrast-enhanced EUS with Doppler mode, contrast-enhanced harmonic EUS, 3-dimensinal EUS, and EUS elastography. Incorporation of these methods has improved the differential diagnosis of pancreatic tumors. Finally, a multi-disciplinary approach involving radiology, gastroenterology and surgical specialties is often necessary for accurate diagnosis and management of solid and cystic pancreatic tumors.
Figures





Similar articles
-
Diagnosis of pancreatic tumors by endoscopic ultrasonography.World J Radiol. 2010 Apr 28;2(4):122-34. doi: 10.4329/wjr.v2.i4.122. World J Radiol. 2010. PMID: 21160578 Free PMC article.
-
Endoscopic ultrasound in solid pancreatic masses--current state and review of the literature.Coll Antropol. 2010 Mar;34(1):337-40. Coll Antropol. 2010. PMID: 20432768 Review.
-
Endoscopic ultrasonography-guided fine-needle aspiration cytology of surgically confirmed cystic pancreatic neuroendocrine tumors: a Mayo Clinic experience.J Am Soc Cytopathol. 2015 Nov-Dec;4(6):335-343. doi: 10.1016/j.jasc.2015.04.001. Epub 2015 Apr 15. J Am Soc Cytopathol. 2015. PMID: 31051748
-
Performance of endosonography-guided fine needle aspiration and biopsy in the diagnosis of pancreatic cystic lesions.Am J Gastroenterol. 2003 Jul;98(7):1516-24. doi: 10.1111/j.1572-0241.2003.07530.x. Am J Gastroenterol. 2003. PMID: 12873573
-
Endoscopic approach to the diagnosis of pancreatic cystic tumor.World J Gastrointest Oncol. 2016 Feb 15;8(2):159-64. doi: 10.4251/wjgo.v8.i2.159. World J Gastrointest Oncol. 2016. PMID: 26909130 Free PMC article. Review.
Cited by
-
Tumors and new endoscopic ultrasound-guided therapies.World J Gastrointest Endosc. 2013 Apr 16;5(4):141-7. doi: 10.4253/wjge.v5.i4.141. World J Gastrointest Endosc. 2013. PMID: 23596535 Free PMC article.
-
Tumor size as measured at initial X-ray examination, not length of bile duct stricture, predicts survival in patients with unresectable pancreatic cancer.BMC Cancer. 2012 Sep 25;12:429. doi: 10.1186/1471-2407-12-429. BMC Cancer. 2012. PMID: 23009736 Free PMC article.
-
Diagnosis and treatment of pancreatic pseudocysts and cystic tumors based on own material and quoted literature.J Ultrason. 2013 Sep;13(54):263-81. doi: 10.15557/JoU.2013.0028. Epub 2013 Sep 30. J Ultrason. 2013. PMID: 26673675 Free PMC article.
-
Effectiveness of contrast-enhanced harmonic endoscopic ultrasound for the evaluation of solid pancreatic masses.World J Gastroenterol. 2014 Jan 14;20(2):518-24. doi: 10.3748/wjg.v20.i2.518. World J Gastroenterol. 2014. PMID: 24574720 Free PMC article.
-
[Value of endoscopic ultrasound-guided fine needle aspiration in pretest prediction and diagnosis of pancreatic ductal adenocarcinoma].Nan Fang Yi Ke Da Xue Xue Bao. 2018 Sep 30;38(10):1171-1178. doi: 10.3969/j.issn.1673-4254.2018.10.04. Nan Fang Yi Ke Da Xue Xue Bao. 2018. PMID: 30377133 Free PMC article. Chinese.
References
-
- Palazzo L, Roseau G, Gayet B, Vilgrain V, Belghiti J, Fekete F, et al. Endoscopic ultrasonography in the diagnosis and staging of pancreatic adenocarcinoma. Results of a prospective study with comparison to ultrasonography and CT scan. Endoscopy. 1993;25:143–150. - PubMed
-
- Khashab MA, Yong E, Lennon AM, Shin EJ, Amateau S, Hruban RH, et al. EUS is still superior to multidetector computerized tomography for detection of pancreatic neuroendocrine tumors. Gastrointestinal endoscopy. 2011;73:691–696. - PubMed
-
- Rosewicz S, Wiedenmann B. Pancreatic carcinoma. Lancet. 1997;349:485–489. - PubMed
-
- Rosch T, Lightdale CJ, Botet JF, Boyce GA, Sivak MV, Jr, Yasuda K, et al. Localization of pancreatic endocrine tumors by endoscopic ultrasonography. N Engl J Med. 1992;326:1721–1726. - PubMed
LinkOut - more resources
Full Text Sources