

Bariatric surgery and T2DM improvement mechanisms: a mathematical model
- PMID: 22587410
- PMCID: PMC3586953
- DOI: 10.1186/1742-4682-9-16
Bariatric surgery and T2DM improvement mechanisms: a mathematical model
Abstract
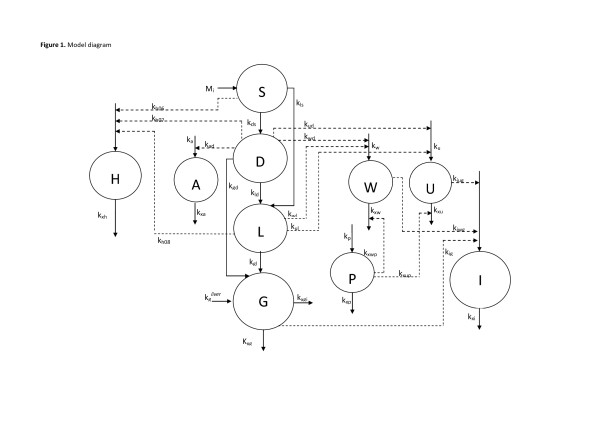
Background: Consensus exists that several bariatric surgery procedures produce a rapid improvement of glucose homeostasis in obese diabetic patients, improvement apparently uncorrelated with the degree of eventual weight loss after surgery. Several hypotheses have been suggested to account for these results: among these, the anti-incretin, the ghrelin and the lower-intestinal dumping hypotheses have been discussed in the literature. Since no clear-cut experimental results are so far available to confirm or disprove any of these hypotheses, in the present work a mathematical model of the glucose-insulin-incretin system has been built, capable of expressing these three postulated mechanisms. The model has been populated with critically evaluated parameter values from the literature, and simulations under the three scenarios have been compared.
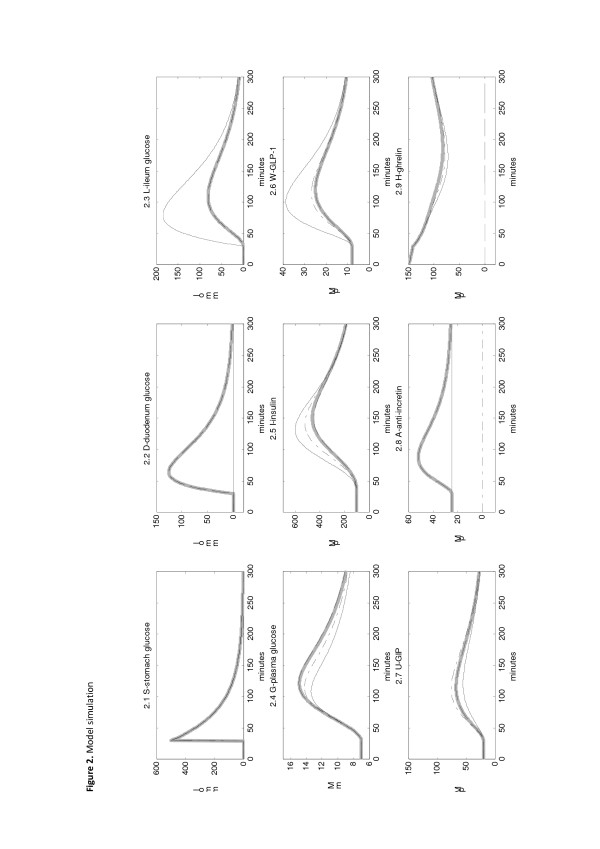
Results: The modeling results seem to indicate that the suppression of ghrelin release is unlikely to determine major changes in short-term glucose control. The possible existence of an anti-incretin hormone would be supported if an experimental increase of GIP concentrations were evident post-surgery. Given that, on the contrary, collected evidence suggests that GIP concentrations decrease post-surgery, the lower-intestinal dumping hypothesis would seem to describe the mechanism most likely to produce the observed normalization of Type 2 Diabetes Mellitus (T2DM) after bariatric surgery.
Conclusions: The proposed model can help discriminate among competing hypotheses in a context where definitive data are not available and mechanisms are still not clear.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
