

Review article: current treatment options and management of functional dyspepsia
- PMID: 22591037
- PMCID: PMC3970847
- DOI: 10.1111/j.1365-2036.2012.05128.x
Review article: current treatment options and management of functional dyspepsia
Abstract
Background: Functional dyspepsia (FD), a common functional gastrointestinal disorder, is defined by the Rome III criteria as symptoms of epigastric pain or discomfort (prevalence in FD of 89-90%), postprandial fullness (75-88%), and early satiety (50-82%) within the last 3 months with symptom onset at least 6 months earlier. Patients cannot have any evidence of structural disease to explain symptoms and predominant symptoms of gastroesophageal reflux are exclusionary. Symptoms of FD are non-specific and the pathophysiology is diverse, which explains in part why a universally effective treatment for FD remains elusive.
Aim: To present current management options for the treatment of FD (therapeutic gain/response rate noted when available).
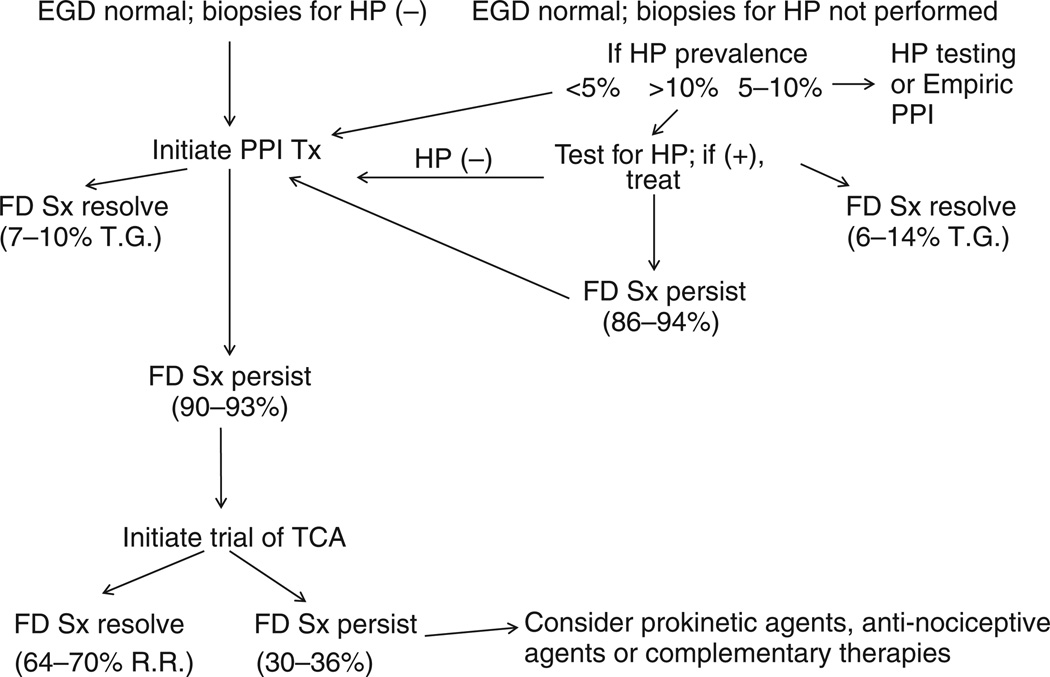
Results: The utility of Helicobacter pylori eradication for the treatment of FD is modest (6-14% therapeutic gain), while the therapeutic efficacy of proton pump inhibitors (PPI) (7-10% therapeutic gain), histamine-type-2-receptor antagonists (8-35% therapeutic gain), prokinetic agents (18-45%), tricyclic antidepressants (TCA) (response rates of 64-70%), serotonin reuptake inhibitors (no better than placebo) is limited and hampered by inadequate data. This review discusses dietary interventions and analyses studies involving complementary and alternative medications, and psychological therapies.
Conclusions: A reasonable treatment approach based on current evidence is to initiate therapy with a daily PPI in H. pylori-negative FD patients. If symptoms persist, a therapeutic trial with a tricyclic antidepressant may be initiated. If symptoms continue, the clinician can possibly initiate therapy with an anti-nociceptive agent, a prokinetic agent, or some form of complementary and alternative medications, although evidence from prospective studies to support this approach is limited.
© 2012 Blackwell Publishing Ltd.
Figures
References
-
- Camilleri M, Dubois D, Coulie B, et al. Prevalence and socioeconomic impact of upper gastrointestinal disorders in the United States: results of the US Upper Gastrointestinal Study. Clin Gastroenterol Hepatol. 2005;3:543–552. - PubMed
-
- El-Serag HB, Talley NJ. Systematic review: the prevalence and clinical course of functional dyspepsia. Aliment Pharmacol Ther. 2004;19:643–654. - PubMed
-
- Castillo EJ, Camilleri M, Locke GR, III, et al. A community-based, controlled study of the epidemiology and pathophysiology of dyspepsia. Clin Gastroenterol Hepatol. 2004;2:985–996. - PubMed
-
- Tack J, Talley NJ, Camilleri M, et al. Functional gastroduodenal disorders. Gastroenterology. 2006;130:1466–1479. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical