

Azithromycin and the risk of cardiovascular death
- PMID: 22591294
- PMCID: PMC3374857
- DOI: 10.1056/NEJMoa1003833
Azithromycin and the risk of cardiovascular death
Abstract
Background: Although several macrolide antibiotics are proarrhythmic and associated with an increased risk of sudden cardiac death, azithromycin is thought to have minimal cardiotoxicity. However, published reports of arrhythmias suggest that azithromycin may increase the risk of cardiovascular death.
Methods: We studied a Tennessee Medicaid cohort designed to detect an increased risk of death related to short-term cardiac effects of medication, excluding patients with serious noncardiovascular illness and person-time during and shortly after hospitalization. The cohort included patients who took azithromycin (347,795 prescriptions), propensity-score-matched persons who took no antibiotics (1,391,180 control periods), and patients who took amoxicillin (1,348,672 prescriptions), ciprofloxacin (264,626 prescriptions), or levofloxacin (193,906 prescriptions).
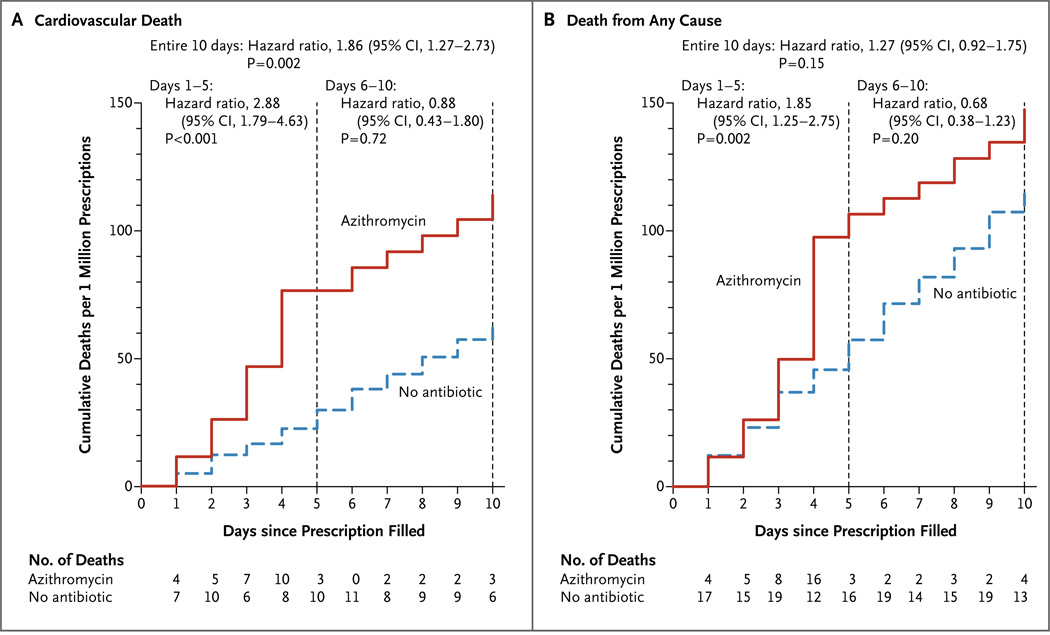
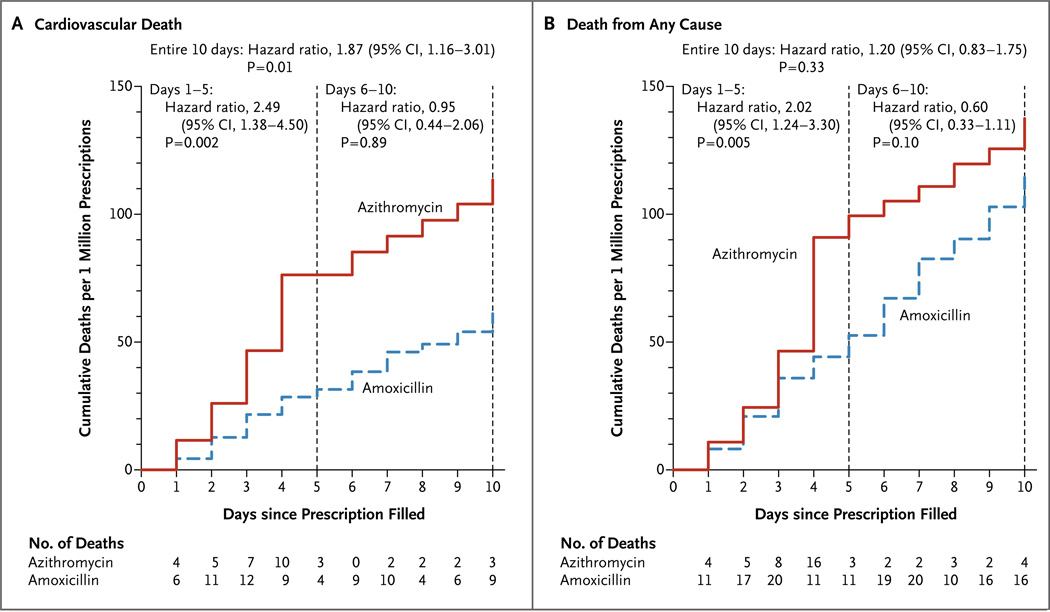
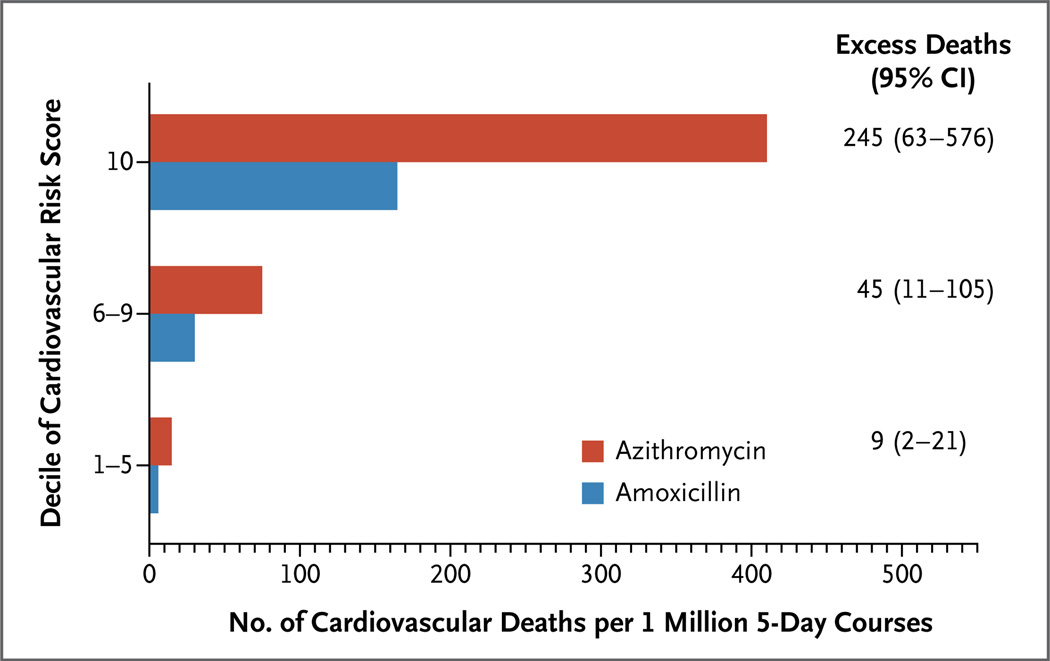
Results: During 5 days of therapy, patients taking azithromycin, as compared with those who took no antibiotics, had an increased risk of cardiovascular death (hazard ratio, 2.88; 95% confidence interval [CI], 1.79 to 4.63; P<0.001) and death from any cause (hazard ratio, 1.85; 95% CI, 1.25 to 2.75; P=0.002). Patients who took amoxicillin had no increase in the risk of death during this period. Relative to amoxicillin, azithromycin was associated with an increased risk of cardiovascular death (hazard ratio, 2.49; 95% CI, 1.38 to 4.50; P=0.002) and death from any cause (hazard ratio, 2.02; 95% CI, 1.24 to 3.30; P=0.005), with an estimated 47 additional cardiovascular deaths per 1 million courses; patients in the highest decile of risk for cardiovascular disease had an estimated 245 additional cardiovascular deaths per 1 million courses. The risk of cardiovascular death was significantly greater with azithromycin than with ciprofloxacin but did not differ significantly from that with levofloxacin.
Conclusions: During 5 days of azithromycin therapy, there was a small absolute increase in cardiovascular deaths, which was most pronounced among patients with a high baseline risk of cardiovascular disease. (Funded by the National Heart, Lung, and Blood Institute and the Agency for Healthcare Quality and Research Centers for Education and Research on Therapeutics.).
Figures
Comment in
-
Azithromycin and the risk of cardiovascular death.N Engl J Med. 2012 Aug 23;367(8):772-3; author reply 775. doi: 10.1056/NEJMc1207269. N Engl J Med. 2012. PMID: 22913693 No abstract available.
-
Azithromycin and the risk of cardiovascular death.N Engl J Med. 2012 Aug 23;367(8):773-4; author reply 775. doi: 10.1056/NEJMc1207269. N Engl J Med. 2012. PMID: 22913694 No abstract available.
-
Azithromycin and the risk of cardiovascular death.N Engl J Med. 2012 Aug 23;367(8):774; author reply 775. doi: 10.1056/NEJMc1207269. N Engl J Med. 2012. PMID: 22913695 No abstract available.
-
Azithromycin and the risk of cardiovascular death.N Engl J Med. 2012 Aug 23;367(8):774; author reply 775. doi: 10.1056/NEJMc1207269. N Engl J Med. 2012. PMID: 22913696 No abstract available.
-
Azithromycin and the risk of cardiovascular death.N Engl J Med. 2012 Aug 23;367(8):774-5; author reply 775. doi: 10.1056/NEJMc1207269. N Engl J Med. 2012. PMID: 22913697 No abstract available.
-
The cardiovascular risk of azithromycin was increased in a large observational cohort study, contradicting findings from prior randomised trials.Evid Based Med. 2013 Jun;18(3):e28. doi: 10.1136/eb-2012-100900. Epub 2012 Sep 5. Evid Based Med. 2013. PMID: 22951814 No abstract available.
-
Cardiovascular risks with azithromycin and other antibacterial drugs.N Engl J Med. 2013 May 2;368(18):1665-8. doi: 10.1056/NEJMp1302726. N Engl J Med. 2013. PMID: 23635046 No abstract available.
References
-
- Owens RC, Jr, Nolin TD. Antimicrobial-associated QT interval prolongation: pointes of interest. Clin Infect Dis. 2006;43:1603–1611. - PubMed
-
- Vogt AW, Zollo RA. Long Q-T syndrome associated with oral erythromycin used in preoperative bowel preparation. Anesth Analg. 1997;85:1011–1013. - PubMed
-
- Tschida SJ, Guay DRP, Straka RJ, Hoey LL, Johanning R, Vance-Bryan K. QTc-interval prolongation associated with slow intravenous erythromycin lactobionate infusions in critically ill patients: a prospective evaluation and review of the literature. Pharmacotherapy. 1996;16:663–674. - PubMed
-
- De Ponti F, Poluzzi E, Montanaro N. QT-interval prolongation by non-cardiac drugs: lessons to be learned from recent experience. Eur J Clin Pharmacol. 2000;56:1–18. - PubMed
-
- Drici MD, Knollmann BC, Wang WX, Woosley RL. Cardiac actions of erythromycin: influence of female sex. JAMA. 1998;280:1774–1776. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical