

Transmitted drug resistance and phylogenetic relationships among acute and early HIV-1-infected individuals in New York City
- PMID: 22592583
- PMCID: PMC3427460
- DOI: 10.1097/QAI.0b013e31825a289b
Transmitted drug resistance and phylogenetic relationships among acute and early HIV-1-infected individuals in New York City
Abstract
Background: Transmitted drug resistance (TDR) is critical to managing HIV-1-infected individuals and being a public health concern. We report on TDR prevalence and include analyses of phylogenetic clustering of HIV-1 in a predominantly men who have sex with men cohort diagnosed during acute/recent HIV-1 infection in New York City.
Methods: Genotypic resistance testing was conducted on plasma samples of 600 individuals with acute/recent HIV-1 infection (1995-2010). Sequences were used for resistance and phylogenetic analyses. Demographic and clinical data were abstracted from medical records. TDR was defined according to International AIDS Society-USA and Stanford HIV database guidelines. Phylogenetic and other analyses were conducted using PAUP*4.0 and SAS, respectively.
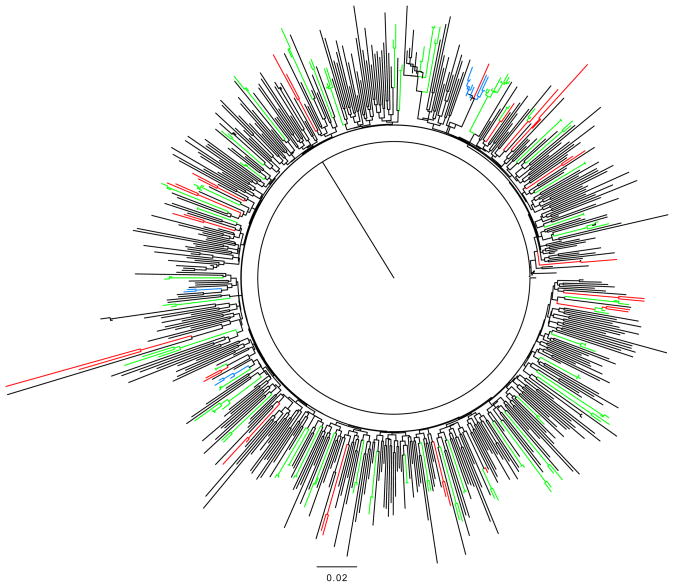
Results: The mean duration since HIV-1 infection was 66.5 days. TDR prevalence was 14.3% and stably ranged between 10.8% and 21.6% (P(trend) = 0.42). Nucleoside reverse transcriptase inhibitors resistance declined from 15.5% to 2.7% over the study period (P(trend) = 0.005). M41L (3.7%), T215Y (4.0%), and K103N/S (4.7%) were the most common mutations. K103N/S prevalence increased from 1.9% to 8.0% between 1995 and 2010 (P(trend) = 0.04). Using a rigorous definition of clustering, 19.3% (112 of 581) of subtype B viral sequences cosegregated into transmission clusters and clusters increased over time. There were fewer and smaller transmission clusters than had been reported in a similar cohort in Montreal but similar to reports from elsewhere.
Conclusions: TDR is stable in this cohort and remains a significant concern to both individual patient management and the public health.
Conflict of interest statement
M. Markowitz has received research funding from Merck, Gilead Sciences, and GlaxoSmithKline. He has been a paid consultant to Merck, Gilead, GlaxoSmithKline, ViiV and Jannsen. He has received honoraria for Speaker’s Bureau participation from Gilead, Bristol-Myers-Squibb and Janssen. For the remaining authors, no conflicts were decleared.
Figures
References
-
- Boden D, Hurley A, Zhang L, Cao Y, Guo Y, Jones E, et al. HIV-1 drug resistance in newly infected individuals. Jama. 1999;282:1135–1141. - PubMed
-
- Simon V, Vanderhoeven J, Hurley A, Ramratnam B, Louie M, Dawson K, et al. Evolving patterns of HIV-1 resistance to antiretroviral agents in newly infected individuals. Aids. 2002;16:1511–1519. - PubMed
-
- Shet A, Berry L, Mohri H, Mehandru S, Chung C, Kim A, et al. Tracking the prevalence of transmitted antiretroviral drug-resistant HIV-1: a decade of experience. J Acquir Immune Defic Syndr. 2006;41:439–446. - PubMed
-
- Dunn DT, Gibb DM, Babiker AG, Green H, Darbyshire JH, Weller IV. HIV drug resistance testing: is the evidence really there? Antivir Ther. 2004;9:641–648. - PubMed
-
- Brenner BG, Roger M, Routy JP, Moisi D, Ntemgwa M, Matte C, et al. High rates of forward transmission events after acute/early HIV-1 infection. J Infect Dis. 2007;195:951–959. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
