

Interventions for smoking cessation in hospitalised patients
- PMID: 22592676
- PMCID: PMC4498489
- DOI: 10.1002/14651858.CD001837.pub3
Interventions for smoking cessation in hospitalised patients
Update in
-
Interventions for smoking cessation in hospitalised patients.Cochrane Database Syst Rev. 2024 May 21;5(5):CD001837. doi: 10.1002/14651858.CD001837.pub4. Cochrane Database Syst Rev. 2024. PMID: 38770804 Free PMC article.
Abstract
Background: Smoking contributes to reasons for hospitalisation, and the period of hospitalisation may be a good time to provide help with quitting.
Objectives: To determine the effectiveness of interventions for smoking cessation that are initiated for hospitalised patients.
Search methods: We searched the Cochrane Tobacco Addiction Group register which includes papers identified from CENTRAL, MEDLINE, EMBASE and PsycINFO in December 2011 for studies of interventions for smoking cessation in hospitalised patients, using terms including (hospital and patient*) or hospitali* or inpatient* or admission* or admitted.
Selection criteria: Randomized and quasi-randomized trials of behavioural, pharmacological or multicomponent interventions to help patients stop smoking, conducted with hospitalised patients who were current smokers or recent quitters (defined as having quit more than one month before hospital admission). The intervention had to start in the hospital but could continue after hospital discharge. We excluded studies of patients admitted to facilities that primarily treat psychiatric disorders or substance abuse, studies that did not report abstinence rates and studies with follow-up of less than six months. Both acute care hospitals and rehabilitation hospitals were included in this update, with separate analyses done for each type of hospital.
Data collection and analysis: Two authors extracted data independently for each paper, with disagreements resolved by consensus.
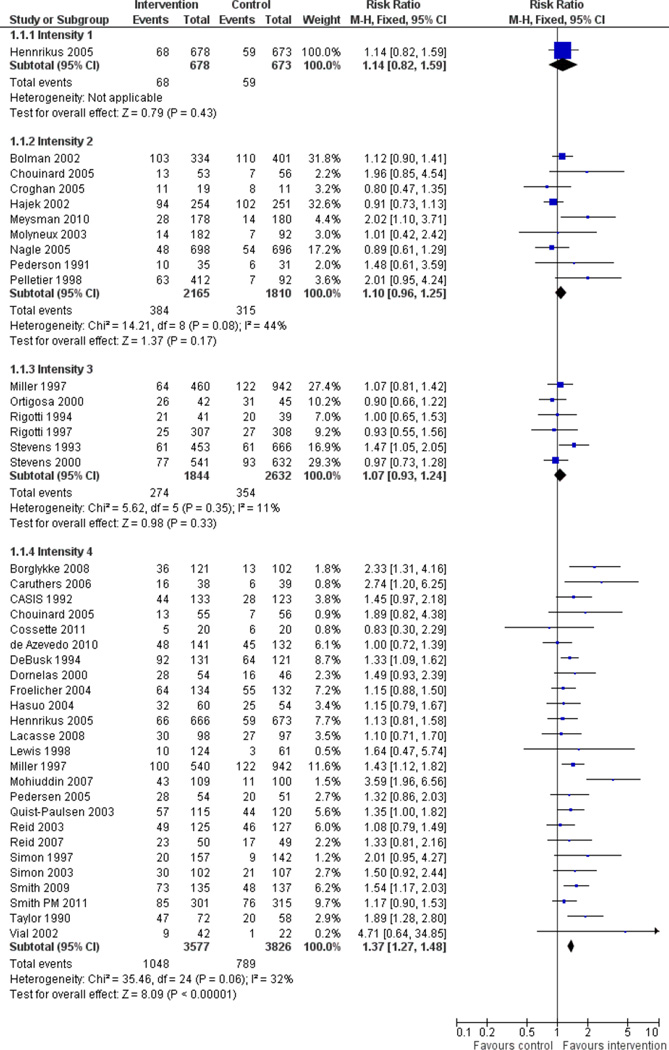
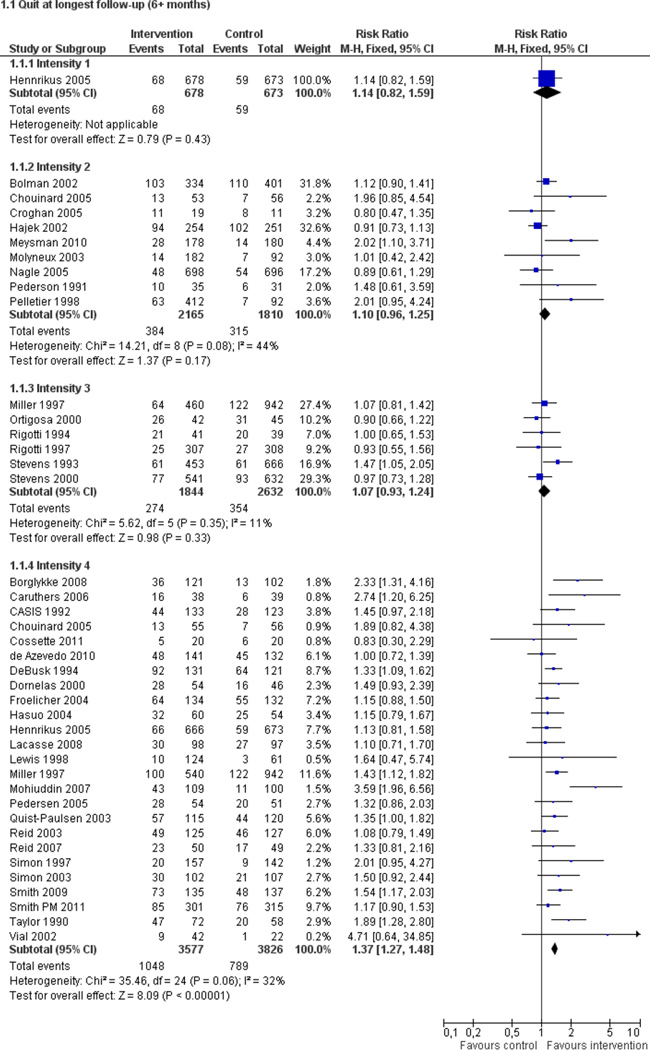
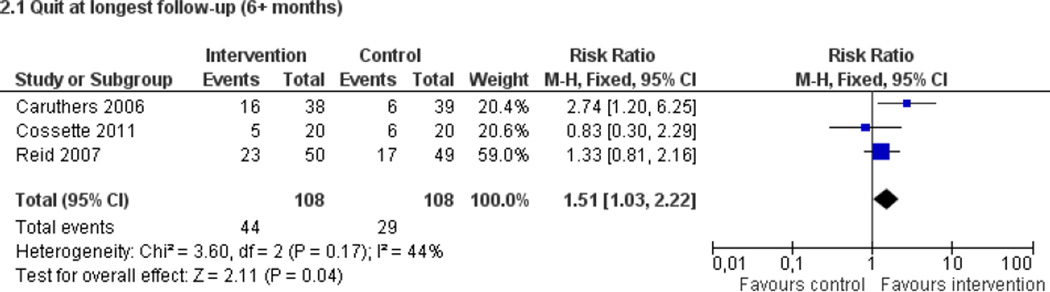
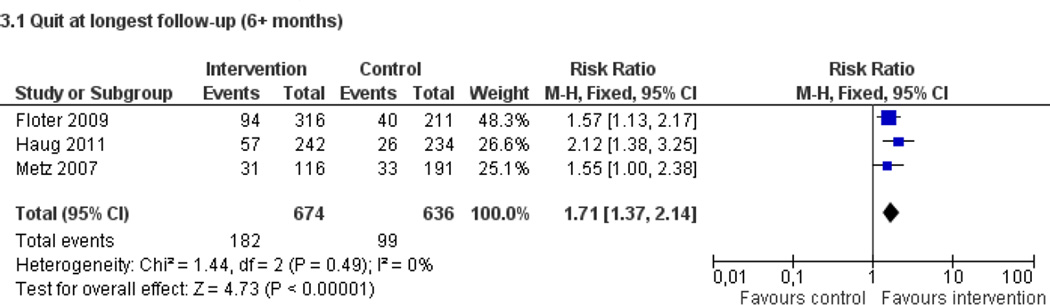
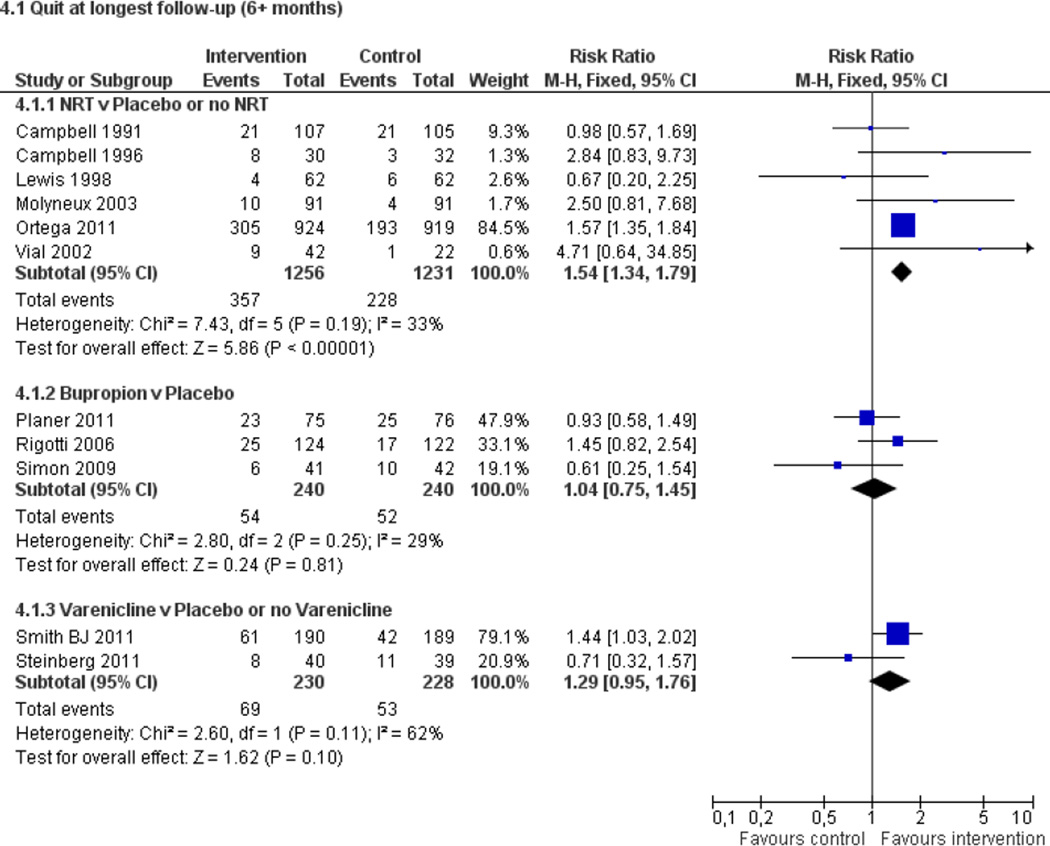
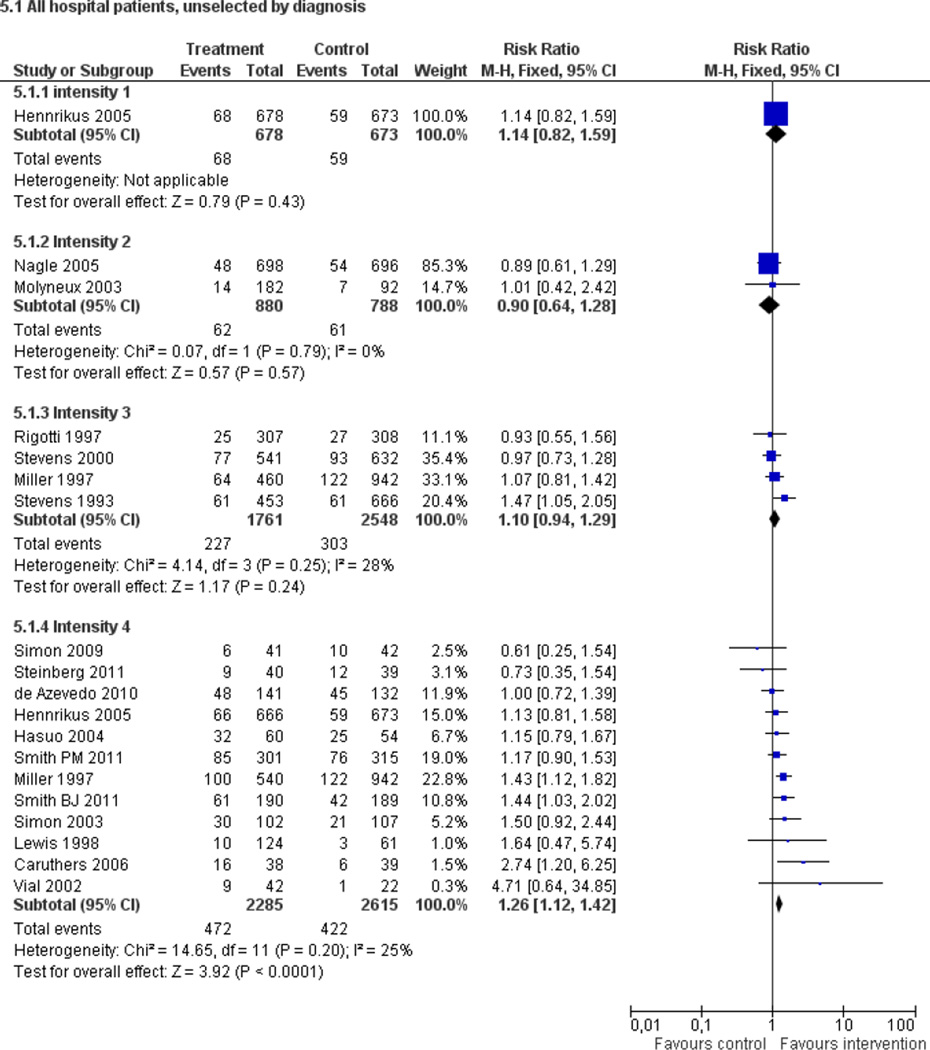
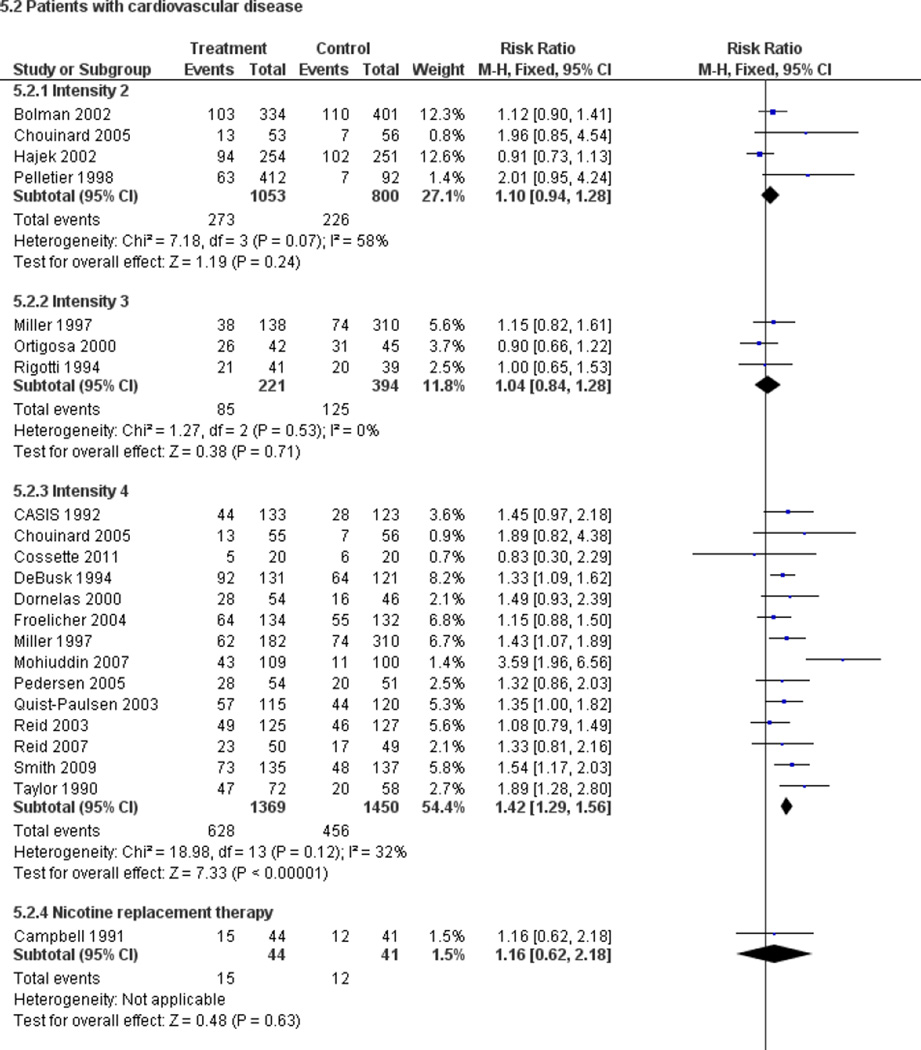
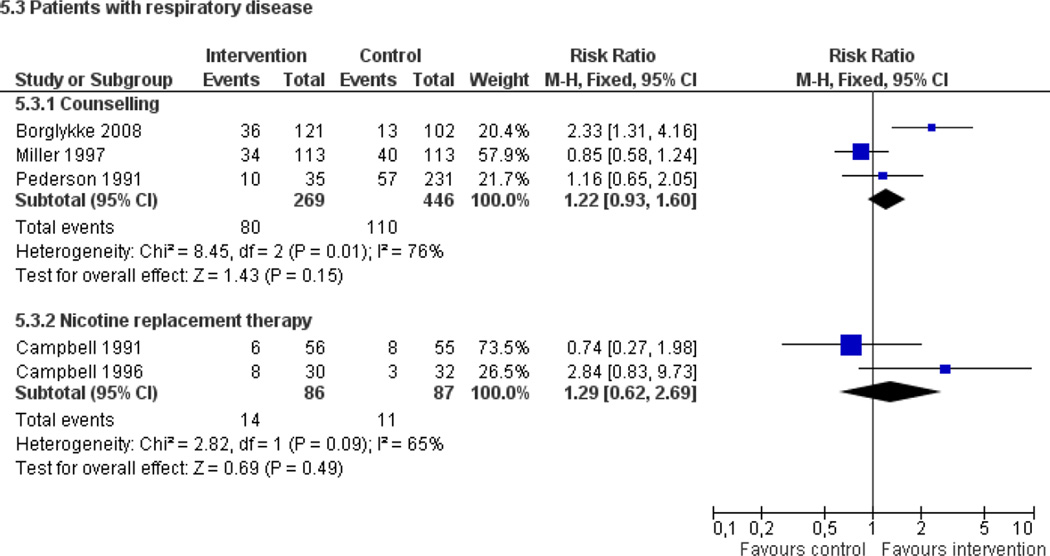
Main results: Fifty trials met the inclusion criteria. Intensive counselling interventions that began during the hospital stay and continued with supportive contacts for at least one month after discharge increased smoking cessation rates after discharge (risk ratio (RR) 1.37, 95% confidence interval (CI) 1.27 to 1.48; 25 trials). A specific benefit for post-discharge contact compared with usual care was found in a subset of trials in which all participants received a counselling intervention in the hospital and were randomly assigned to post-discharge contact or usual care. No statistically significant benefit was found for less intensive counselling interventions. Adding nicotine replacement therapy (NRT) to an intensive counselling intervention increased smoking cessation rates compared with intensive counselling alone (RR 1.54, 95% CI 1.34 to 1.79, six trials). Adding varenicline to intensive counselling had a non-significant effect in two trials (RR 1.28, 95% CI 0.95 to 1.74). Adding bupropion did not produce a statistically significant increase in cessation over intensive counselling alone (RR 1.04, 95% CI 0.75 to 1.45, three trials). A similar pattern of results was observed in a subgroup of smokers admitted to hospital because of cardiovascular disease (CVD). In this subgroup, intensive intervention with follow-up support increased the rate of smoking cessation (RR 1.42, 95% CI 1.29 to 1.56), but less intensive interventions did not. One trial of intensive intervention including counselling and pharmacotherapy for smokers admitted with CVD assessed clinical and health care utilization endpoints, and found significant reductions in all-cause mortality and hospital readmission rates over a two-year follow-up period. These trials were all conducted in acute care hospitals. A comparable increase in smoking cessation rates was observed in a separate pooled analysis of intensive counselling interventions in rehabilitation hospitals (RR 1.71, 95% CI 1.37 to 2.14, three trials).
Authors' conclusions: High intensity behavioural interventions that begin during a hospital stay and include at least one month of supportive contact after discharge promote smoking cessation among hospitalised patients. The effect of these interventions was independent of the patient's admitting diagnosis and was found in rehabilitation settings as well as acute care hospitals. There was no evidence of effect for interventions of lower intensity or shorter duration. This update found that adding NRT to intensive counselling significantly increases cessation rates over counselling alone. There is insufficient direct evidence to conclude that adding bupropion or varenicline to intensive counselling increases cessation rates over what is achieved by counselling alone.
Figures
Update of
-
Interventions for smoking cessation in hospitalised patients.Cochrane Database Syst Rev. 2007 Jul 18;(3):CD001837. doi: 10.1002/14651858.CD001837.pub2. Cochrane Database Syst Rev. 2007. Update in: Cochrane Database Syst Rev. 2012 May 16;(5):CD001837. doi: 10.1002/14651858.CD001837.pub3. PMID: 17636688 Updated.
Comment in
-
Smoking cessation for hospitalised patients: intensive behavioural counselling started in hospital and continued after discharge increases quit rates; with additional benefit from adding nicotine replacement therapy.Evid Based Nurs. 2013 Jan;16(1):21-2. doi: 10.1136/eb-2012-100890. Epub 2012 Sep 8. Evid Based Nurs. 2013. PMID: 22961882 No abstract available.
-
High-intensity interventions promote smoking cessation among hospitalized patients.Evid Based Med. 2013 Jun;18(3):e25. doi: 10.1136/eb-2012-100879. Epub 2012 Sep 21. Evid Based Med. 2013. PMID: 23002093 No abstract available.
References
References to studies
Included studies
-
- Bolman C, De Vries H, van Breukelen G. A minimal-contact intervention for cardiac inpatients: long-term effects on smoking cessation. Preventive Medicine. 2002;35:181–192. - PubMed
-
- Bolman C, de Vries H, Van Breukelen G. Evaluation of a nurse-managed minimal-contact smoking cessation intervention for cardiac inpatients. Health Education Research. 2002;17:99–116. - PubMed
-
- Spencer L, Anderson DRE. A minimal-contact intervention for cardiac inpatients: Long-term effects on smoking cessation. American Journal of Health Promotion. 2004;18:399–400.
-
- Borglykke A, Pisinger C, Jorgensen T, Ibsen H. The effectiveness of smoking cessation groups offered to hospitalised patients with symptoms of exacerbations of chronic obstructive pulmonary disease (COPD) The Clinical Respiratory Journal. 2008;2(3):158–165. - PubMed
-
- Campbell IA, Prescott RJ, Tjeder-Burton SM. Smoking cessation in hospital patients given repeated advice plus nicotine or placebo chewing gum. Respiratory Medicine. 1991;85:155–157. - PubMed
Excluded studies
-
- Agewall S, Fagerberg B, Berglund G, Schmidt C, Wendelhag I, Wikstrand J. Multiple risk intervention trial in high risk hypertensive men: comparison of ultrasound intima-media thickness and clinical outcome during 6 years of follow-up. Journal of Internal Medicine. 2001;249(4):305–314. - PubMed
-
- Asfar T, Ward KD, Vander Weg MW, Hammal F, Eissenberg T, Maziak W. Characteristics of completers and dropouts in Syria's first smoking cessation trial [POS2-132]. Society for Research on Nicotine and Tobacco 11th Annual Meeting; 20–23 March 2005; Prague, Czech Republic. 2005. p. 110.
-
- Avanzini F, Di GP, Amodeo R, Baldo S, Bergna ML, Busi Gal. Effectiveness of a nurse-led educational intervention for patients admitted for acute coronary syndrome. [Italian] Assistenza Infermieristica e Ricerca:Air. 2011;30(1):16–23. - PubMed
-
- Becker BM, Bock BC, Partridge R. Smoking cessation interventions in the emergency department for smokers with chest pain. Academic Emergency Medicine. 2003;10(5):507.
Studies awaiting classification
-
- Brunner-Frandsen NS, Bak S. Smoking cessation intervention after stroke or transient ischemic attack. A randomised controlled trial. Cerebrovascular Diseases. 2010;29(323) - PubMed
-
- Jimenez G, Lopez J, Martinez M, Romero A, Gil B, de Dios LJ, et al. Effectiveness of a specialised intervention for smoking cessation in hospitalised patients [Abstract] European Respiratory Journal. 2007;30(Suppl 51):502s.
Ongoing studies
Other references
Additional references
-
- Cahill K, Stead LF, Lancaster T. Nicotine receptor partial agonists for smoking cessation. Cochrane Database of Systematic Reviews. 2012 Art. No.: CD006103. - PubMed
-
- Higgins JPT, Green S, editors. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0. The Cochrane Collaboration; 2011. [updated March 2011]. available from www.cochrane-handbook.org.
-
- Hughes JR, Stead LF, Lancaster T. Antidepressants for smoking cessation. Cochrane Database of Systematic Reviews. 2007;(1) Art. No.: CD000031. - PubMed
-
- Ladapo JA, Jaffer FA, Weinstein MC, Froelicher ES. Projected cost-effectiveness of smoking cessation interventions in patients hospitalized with myocardial infarction. Archives of Internal Medicine. 2011;171(1):39–45. - PubMed
Other published versions of this review
-
- Rigotti NA, Munafo MR, Murphy MF, Stead LF. Interventions for smoking cessation in hospitalised patients. Cochrane Database of Systematic Reviews. 2001;(2) Art. No.: CD001837. - PubMed
-
- Rigotti NA, Munafo MR, Murphy MF, Stead LF. Interventions for smoking cessation in hospitalised patients. Cochrane Database of Systematic Reviews. 2003;(1) Art. No.: CD001837. - PubMed
-
- Rigotti N, Munafò MR, Stead LF. Interventions for smoking cessation in hospitalised patients. Cochrane Database of Systematic Reviews. 2007;(3) Art. No.: CD001837. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous