

Tissue-engineered vascular grafts for use in the treatment of congenital heart disease: from the bench to the clinic and back again
- PMID: 22594331
- PMCID: PMC3384697
- DOI: 10.2217/rme.12.12
Tissue-engineered vascular grafts for use in the treatment of congenital heart disease: from the bench to the clinic and back again
Abstract
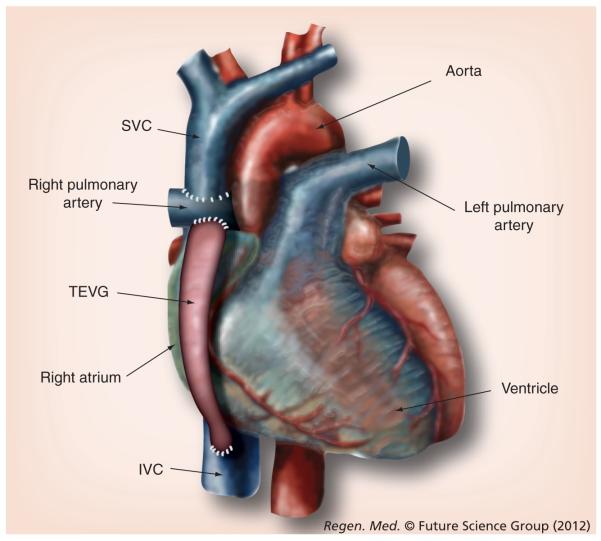
Since the first tissue-engineered vascular graft (TEVG) was implanted in a child over a decade ago, growth in the field of vascular tissue engineering has been driven by clinical demand for improved vascular prostheses with performance and durability similar to an autologous blood vessel. Great strides were made in pediatric congenital heart surgery using the classical tissue engineering paradigm, and cell seeding of scaffolds in vitro remained the cornerstone of neotissue formation. Our second-generation bone marrow cell-seeded TEVG diverged from tissue engineering dogma with a design that induces the recipient to regenerate vascular tissue in situ. New insights suggest that neovessel development is guided by cell signals derived from both seeded cells and host inflammatory cells that infiltrate the graft. The identification of these signals and the regulatory interactions that influence cell migration, phenotype and extracellular matrix deposition during TEVG remodeling are yielding a next-generation TEVG engineered to guide neotissue regeneration without the use of seeded cells. These developments represent steady progress towards our goal of an off-the-shelf tissue-engineered vascular conduit for pediatric congenital heart surgery.
Figures
References
-
- Connelly M, Webb G, Somerville J, et al. Canadian consensus conference on adult congenital heart disease 1996. Can. J. Cardiol. 1998;14(3):395–452. - PubMed
-
- Webb CL, Jenkins KJ, Karpawich PP, et al. Collaborative care for adults with congenital heart disease. Circulation. 2002;105(19):2318–2323. - PubMed
-
- Hager A, Kaemmerer H, Eicken A, Fratz S, Hess J. Long-term survival of patients with univentricular heart not treated surgically. J. Thorac. Cardiovasc. Surg. 2002;123(6):1214–1217. - PubMed
-
- Samánek M. Children with congenital heart disease: probability of natural survival. Pediatr. Cardiol. 1992;13(3):152–158. - PubMed
Websites
-
- The Children’s Heart Foundation fact sheets. http://childrensheartfoundation.org.
-
- Breuer C. NCT01034007: a pilot study investigating the clinical use of tissue engineered vascular grafts in congenital heart surgery. http://clinicaltrials.gov/ct2/show/NCT01034007.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical