

Assessment of lymph node status in gallbladder cancer: location, number, or ratio of positive nodes
- PMID: 22594526
- PMCID: PMC3532237
- DOI: 10.1186/1477-7819-10-87
Assessment of lymph node status in gallbladder cancer: location, number, or ratio of positive nodes
Abstract
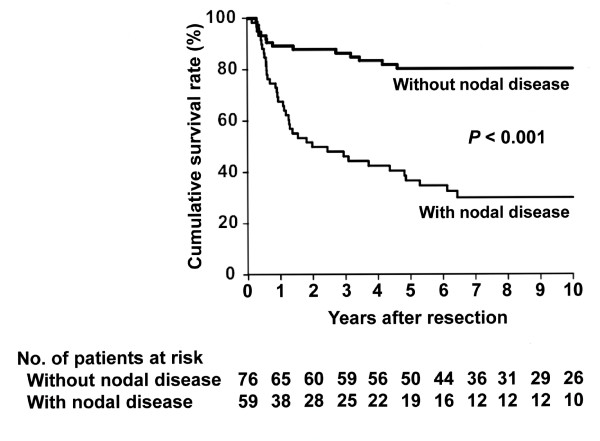
A BACKGROUND: Assessment of lymph node status is a critical issue in the surgical management of gallbladder cancer. The aim of this study was to compare the anatomical location of positive nodes, number of positive nodes, and lymph node ratio (LNR) as prognostic predictors in gallbladder cancer.
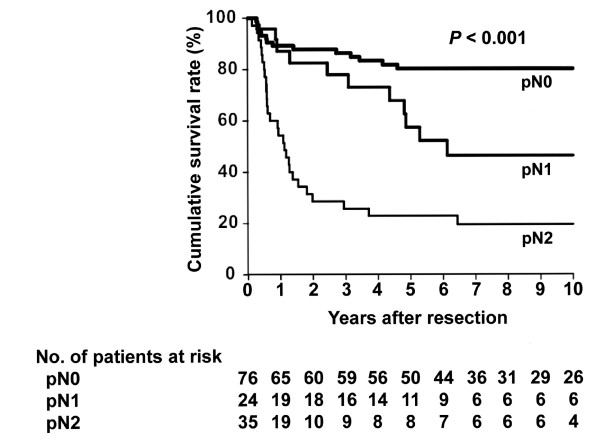
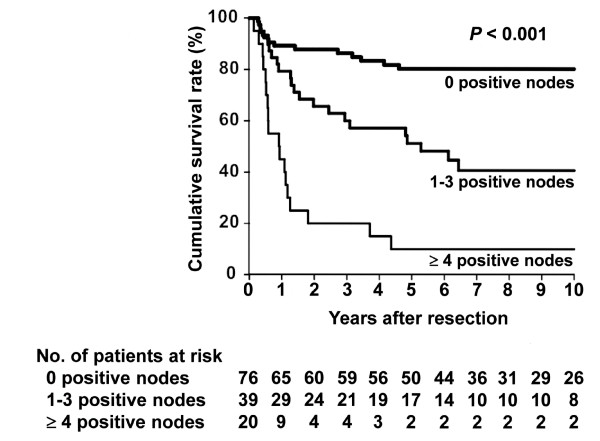
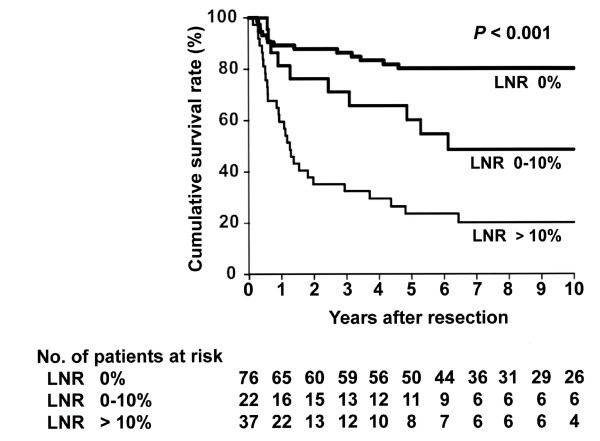
Methods: We conducted a retrospective analysis of 135 patients with gallbladder cancer who underwent a radical resection with regional lymphadenectomy. A total of 2,245 regional lymph nodes were retrieved (median, 14 per patient). The location of positive nodes was classified according to the AJCC staging manual (7th edition). 'Optimal' cutoff values were determined for the number of positive nodes and LNR based on maximal χ(2) scores calculated with the Cox proportional hazards regression model.
Results: Lymph node metastasis was found histologically in 59 (44%) patients. The 'optimal' cutoff values for the number of positive nodes and LNR were determined to be three nodes and 10%, respectively. Univariate analysis identified location of positive nodes (pN0, pN1, pN2; P<0.001), number of positive nodes (0, 1 to 3, ≥ 4; P <0.001), and LNR (0%, 0 to 10%, >10%; P<0.001) as significant prognostic factors. Multivariate analysis identified number of positive nodes as an independent prognostic factor ( P=0.004); however, location of positive nodes and LNR failed to remain as an independent variable.
Conclusions: The number of positive lymph nodes better predicts patient outcome after resection than either the location of positive lymph nodes or LNR in gallbladder cancer. Dividing the number of positive lymph nodes into three categories (0, 1 to 3, or ≥ 4) is valid for stratifying patients based on the prognosis after resection.
Figures
References
-
- Marchet A, Mocellin S, Ambrosi A, Morgagni P, Garcea D, Marrelli D, Roviello F, de Manzoni G, Minicozzi A, Natalini G, De Santis F, Baiocchi L, Coniglio A, Nitti D. The ratio between metastatic and examined lymph nodes (N Ratio) is an independent prognostic factor in gastric cancer regardless of the type of lymphadenectomy: results from an Italian multicentric study in 1853 patients. Ann Surg. 2007;245:543–552. doi: 10.1097/01.sla.0000250423.43436.e1. - DOI - PMC - PubMed
-
- Maduekwe UN, Lauwers GY, Fernandez-Del-Castillo C, Berger DL, Ferguson CM, Rattner DW, Yoon SS. New metastatic lymph node ratio system reduces stage migration in patients undergoing D1 lymphadenectomy for gastric adenocarcinoma. Ann Surg Oncol. 2010;17:1267–1277. doi: 10.1245/s10434-010-0914-6. - DOI - PMC - PubMed
-
- Murakami Y, Uemura K, Sudo T, Hayashidani Y, Hashimoto Y, Nakashima A, Yuasa Y, Kondo N, Ohge H, Sueda T. Number of metastatic lymph nodes, but not lymph node ratio, is an independent prognostic factor after resection of pancreatic carcinoma. J Am Coll Surg. 2010;211:196–204. doi: 10.1016/j.jamcollsurg.2010.03.037. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
